Download as PDF, PPTX

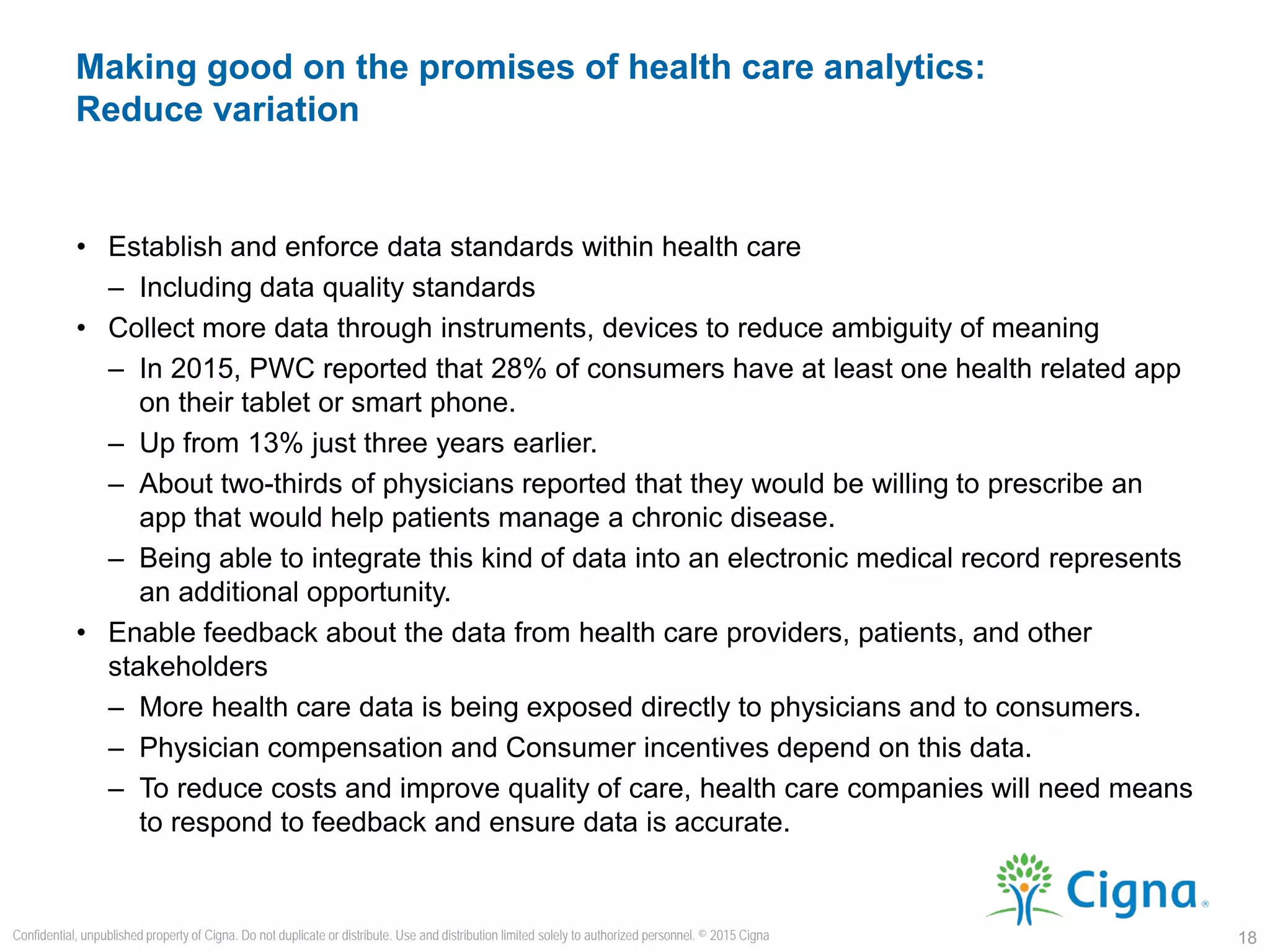
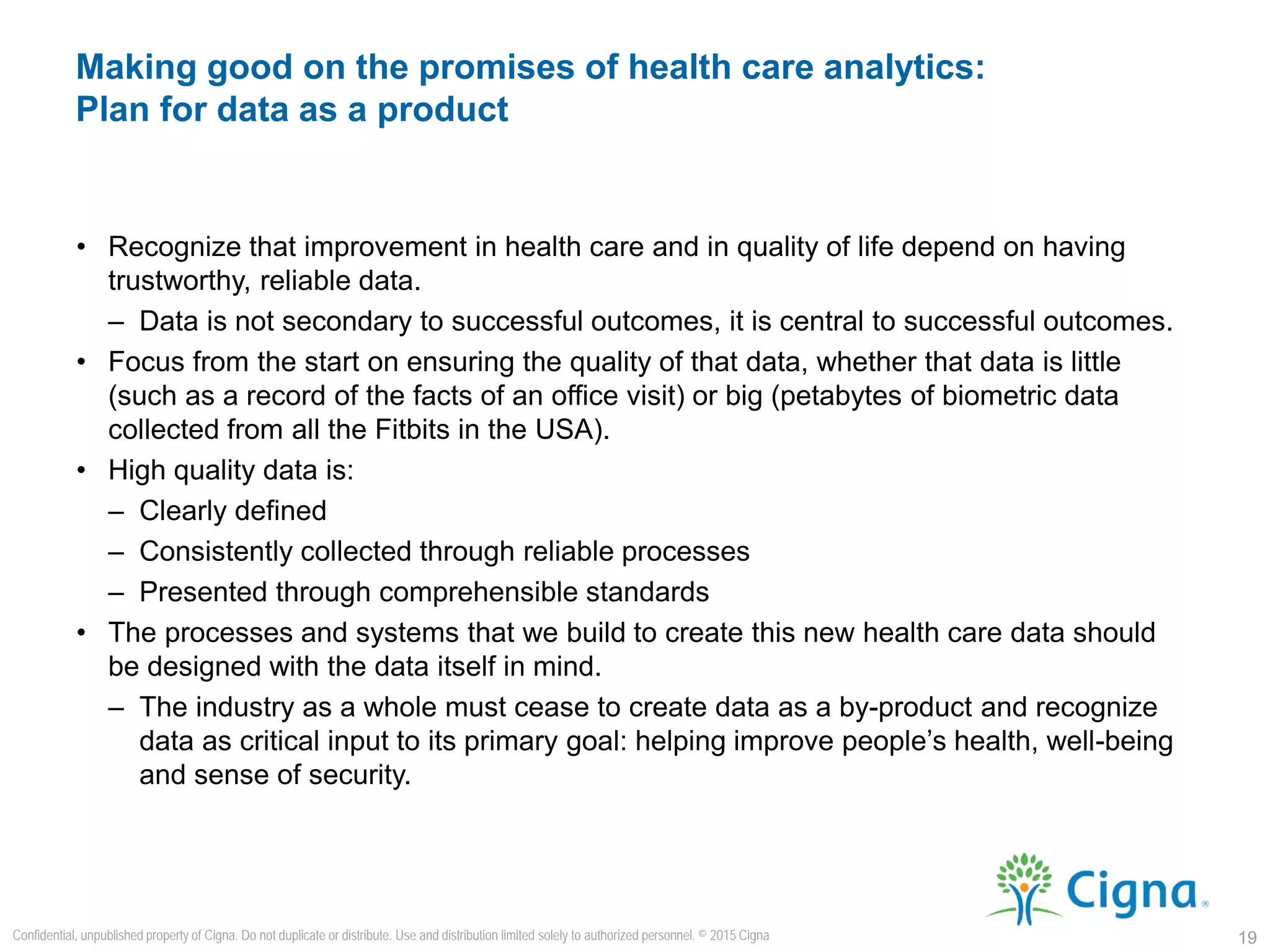























The document discusses the challenges of ensuring high quality data in the healthcare sector amidst the promise of big data analytics, emphasizing that organizational inefficiencies and varying coding practices can compromise data integrity. It advocates for recognizing data as a critical component for successful health outcomes and the need for consistent data standards to enhance analysis and decision-making in clinical settings. Overall, the presentation calls for a shift in mindset regarding data quality, highlighting its importance for effective healthcare delivery and improved patient outcomes.












![[DSC Europe 22] Lakehouse architecture with Delta Lake and Databricks - Draga...](https://cdn.slidesharecdn.com/ss_thumbnails/draganberic-lakehousearchitecturewithdeltalakeanddatabricks-221130080712-6e817e95-thumbnail.jpg?width=640&height=640&fit=bounds)
















![Big Data [sorry] & Data Science: What Does a Data Scientist Do?](https://cdn.slidesharecdn.com/ss_thumbnails/dslatcloudmsevent20130125-130126065651-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)








































































