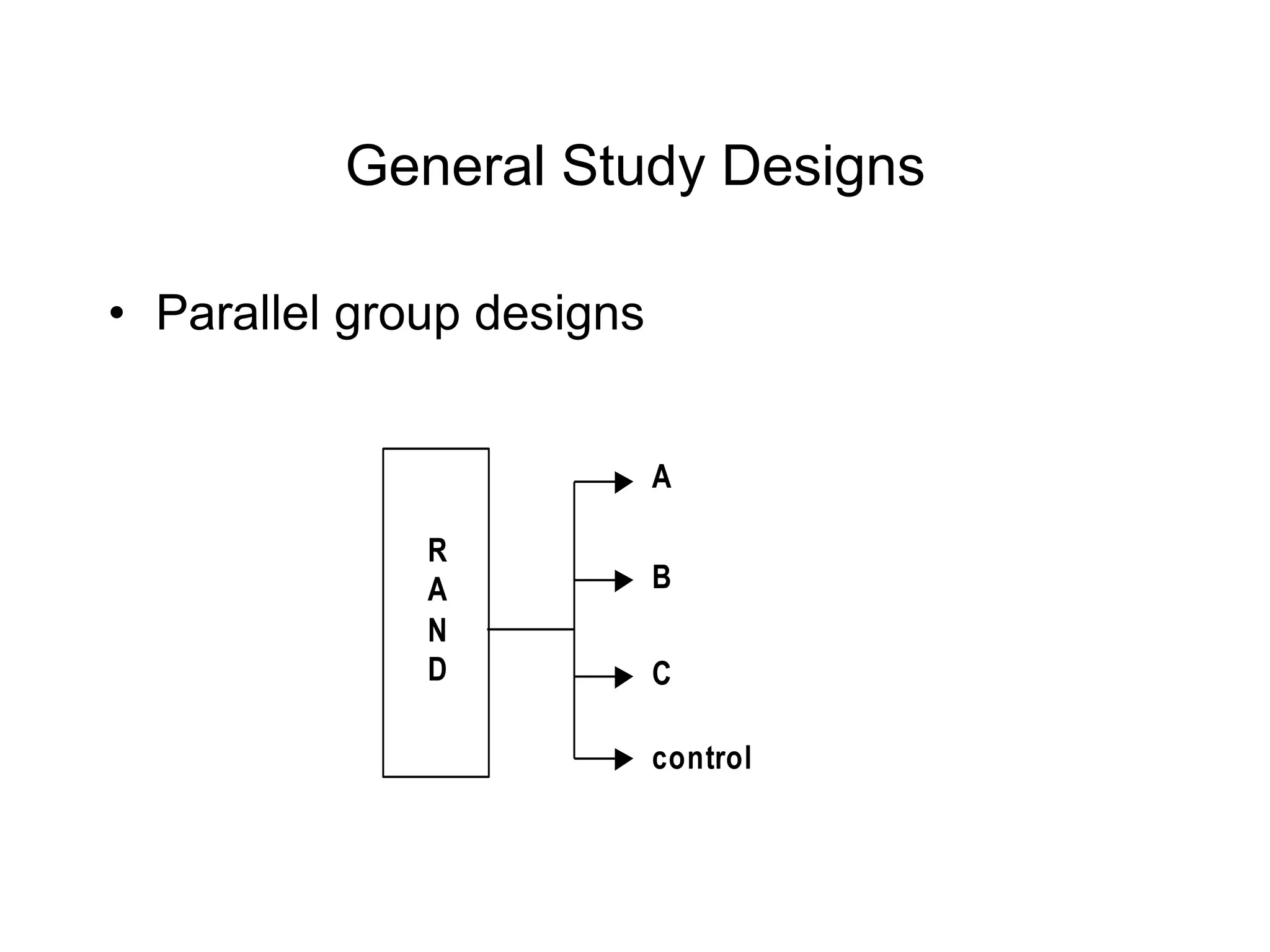
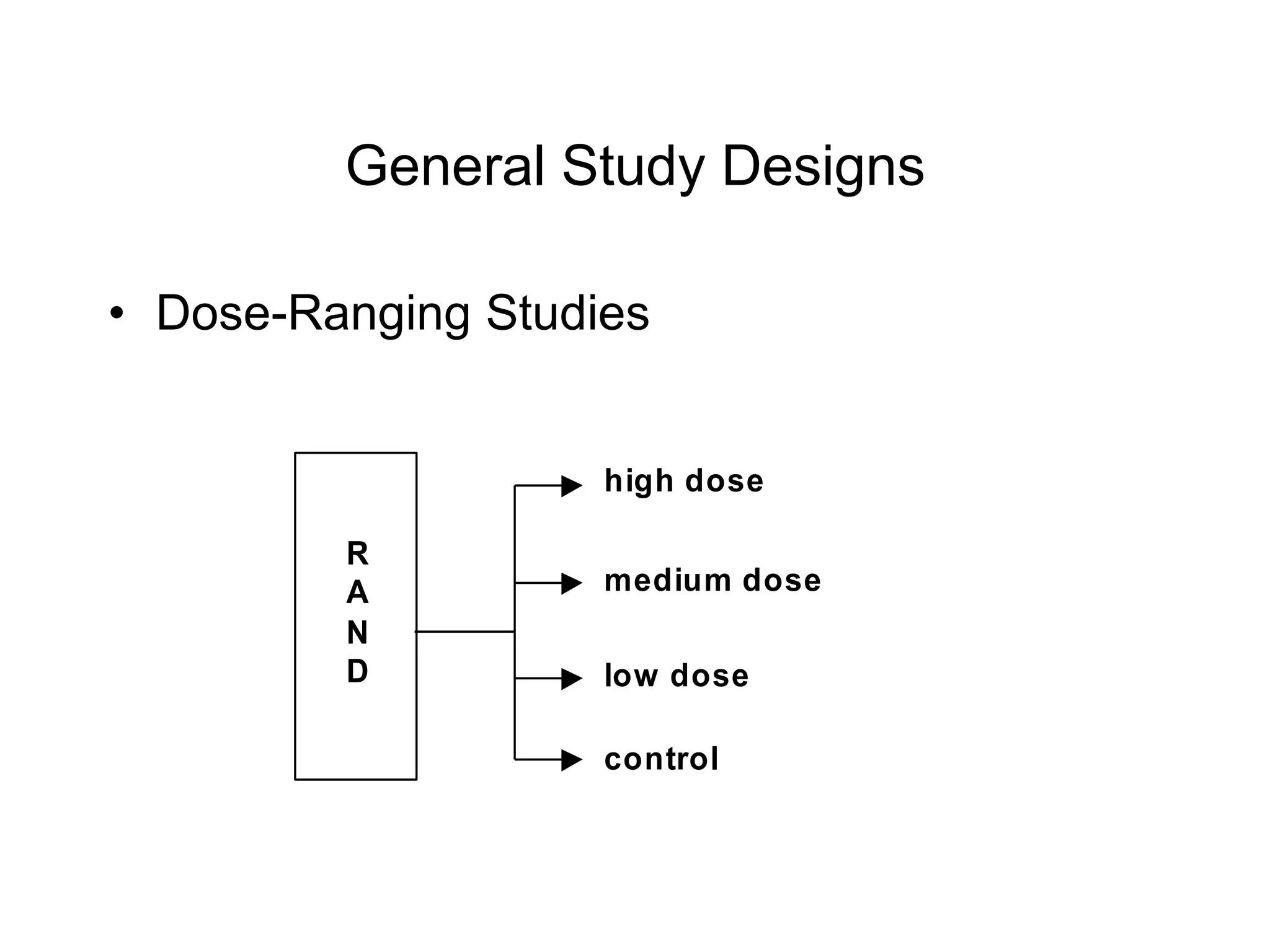
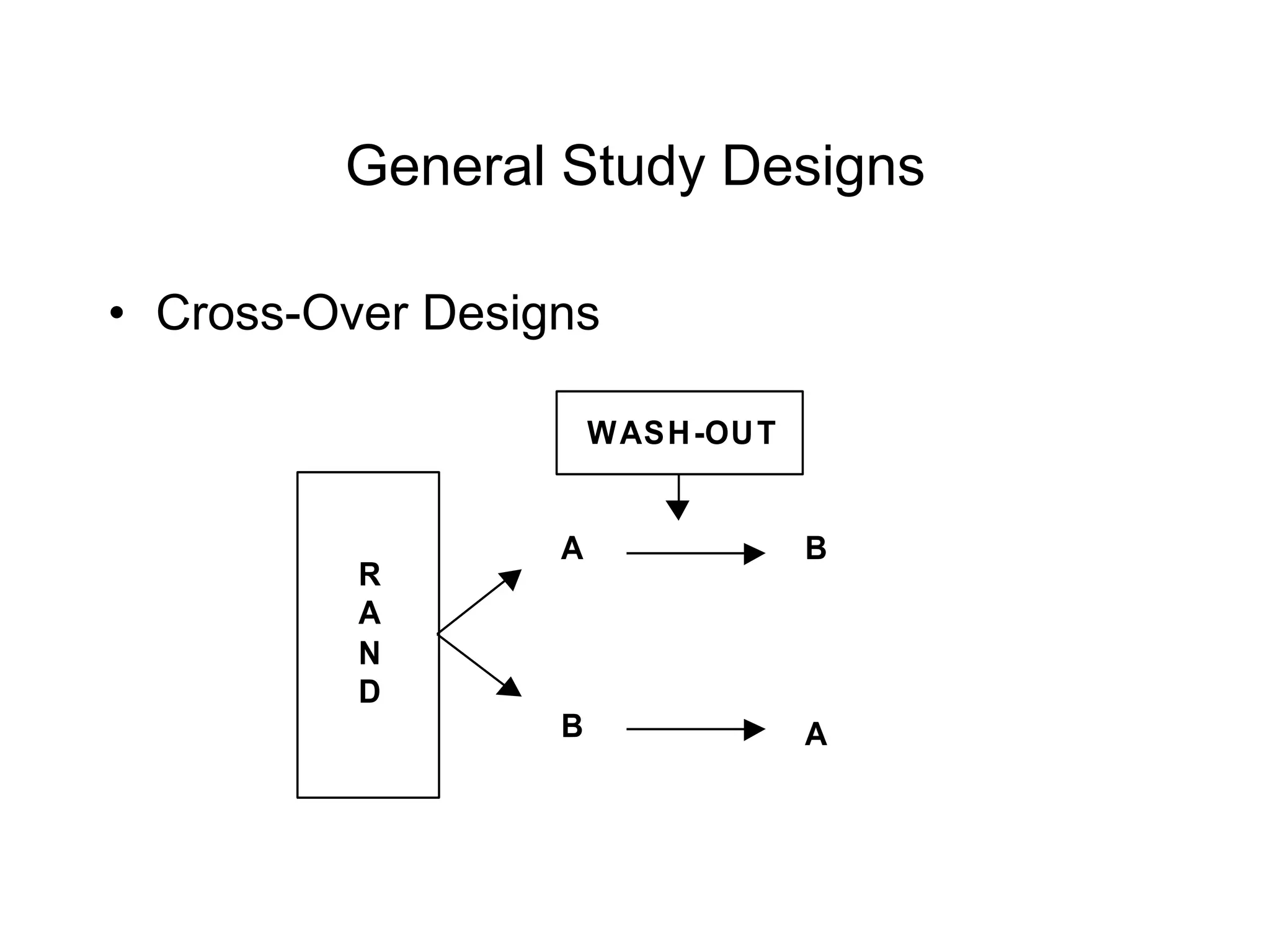
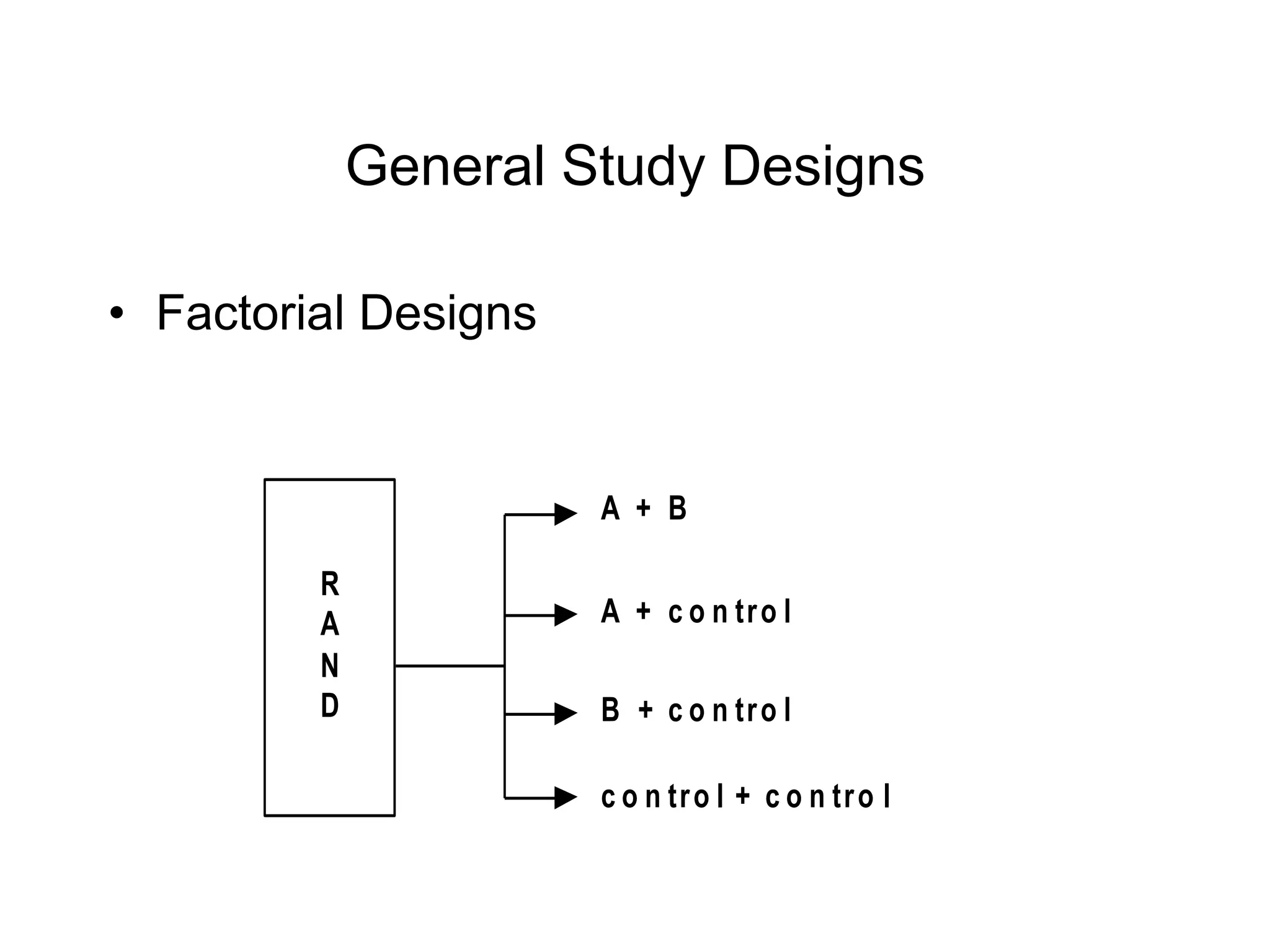
This document provides an overview of key concepts in study design, including bias, variability, randomization, blinding, and common study designs such as parallel group, dose-ranging, cross-over, and factorial designs. Randomization and blinding help reduce bias and ensure comparable treatment groups. Common study designs include parallel group, where subjects are randomly assigned to different treatment groups; dose-ranging, where subjects are assigned varying doses of a treatment; cross-over, where subjects receive multiple treatments in a defined order; and factorial designs, which evaluate multiple interventions simultaneously.