Urology & NephrologyCenter
Mansoura University
Introduction
• Systemic lupus erythematosus (SLE) is an autoimmune disease that causes
chronic inflammation and damage to multiple organs.
• A common and severe manifestation of SLE that requires evaluation is kidney
involvement, referred to as “lupus nephritis”.
• Monitoring kidney function in patients with SLE is crucial, as early detection
and management of renal impairment can significantly improve outcomes.
5.
Urology & NephrologyCenter
Mansoura University
Epidemiology
• SLE can affect individuals of any age, gender, or ethnicity, but it is most
common in women of childbearing age.
50% of patients with SLE develop nephritis
• Risk factors:
1. Younger age.
2. Male sex.
3. Non-European ethnicity.
6.
Urology & NephrologyCenter
Mansoura University
Epidemiology
• Timing:
early in the disease course: first 6-36 months, may be at the initial diagnosis.
• Mortality:
higher in those with lupus nephritis.
Urology & NephrologyCenter
Mansoura University
Diagnosis
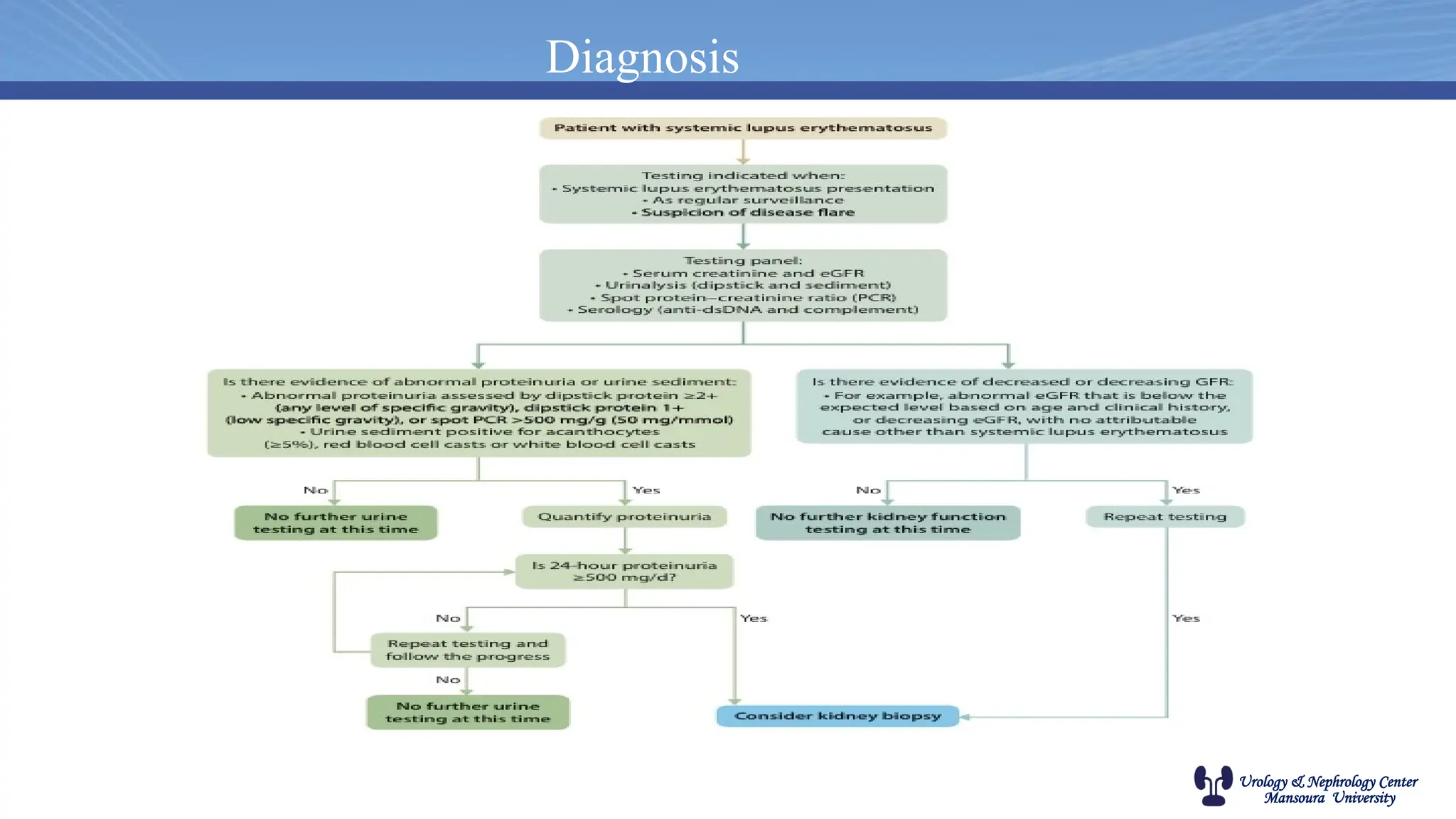
All patients with SLE should be evaluated for kidney involvement:
1. At initial diagnosis.
2. Every 3-6 months.
3. SLE flare.
Urology & NephrologyCenter
Mansoura University
Diagnosis
Renal biopsy in SLE
Indications for biopsy include:
Persistent proteinuria > 0.5 g/day.
Glomerular hematuria.
Unexplained fall in estimated GFR (eGFR).
Urology & NephrologyCenter
Mansoura University
UNC protocol
Non-immunosuppressive therapy
It includes: 1-diet advice
2-diuretics for edema
3-ACEi or ARBs for proteinuria,
4-statin for dyslipidemia
5-vaccinations
6-aspirin or warfarin (if there is anti-phospholipid syndrome)
7-hydroxychloroquine
Immunosuppressive therapy(Allow for reasonable time before escalation to more aggressive regimens
especially in partial responders)
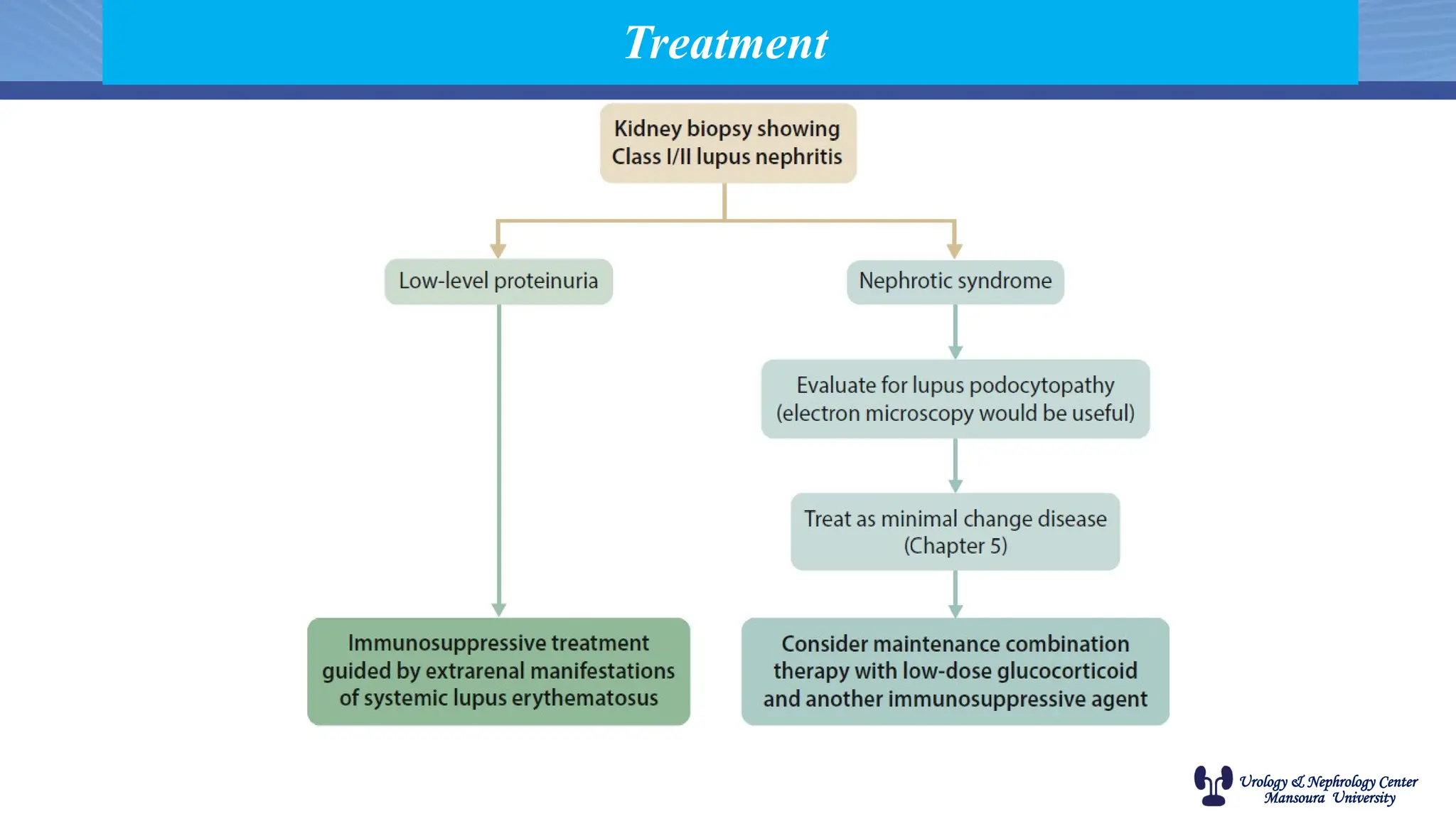
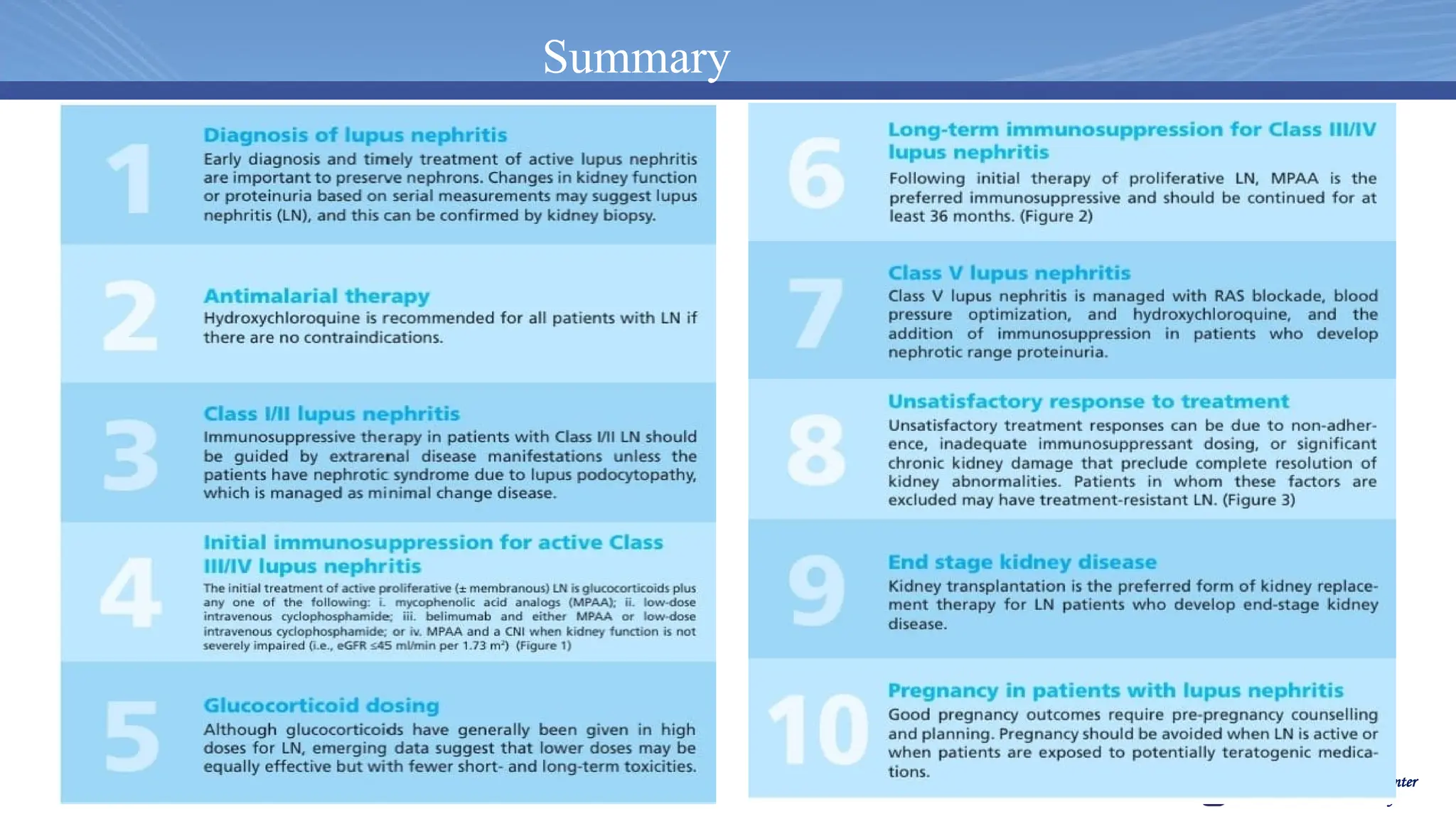
Class I and II lupus nephritis
o Without nephrotic syndrome: As dictated by extra-renal manifestations
o With nephrotic syndrome: As minimal change disease
Urology & NephrologyCenter
Mansoura University
UNC protocol
Focal and diffuse proliferative lupus nephritis
o Severe active disease (rapidly progressive glomerulonephritis and/or severe extra-renal
disease):
Methylprednisolone IV 0.5 g/day for 5 days followed by therapy as in “mild to moderate
active disease”
o Mild to moderate active disease: Induction therapy for 6 months:
Prednisolone 60 mg/day oral for 2-3 months which is then tapered (depending on the
clinical situation) over the subsequent 3-6 months till the dose becomes 10-15 mg/day;
AND
EITHER MMF 2-3 gram/day for 6 months
OR cyclophosphamide IV pulses 500 mg every 2 weeks for 6 doses followed by MMF 2
g/day 2 weeks after the 6th cyclophosphamide dose
37.
Urology & NephrologyCenter
Mansoura University
UNC protocol
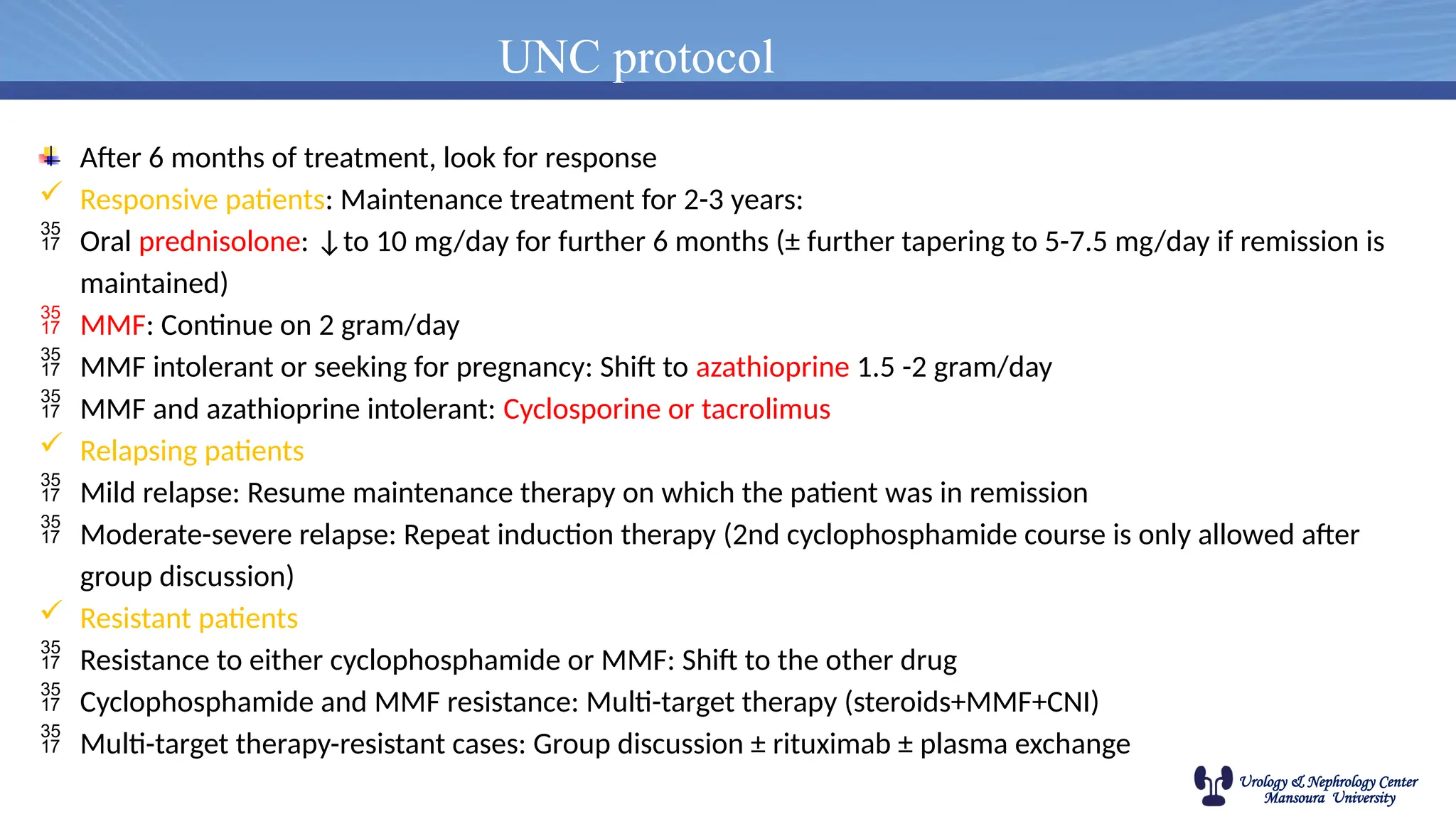
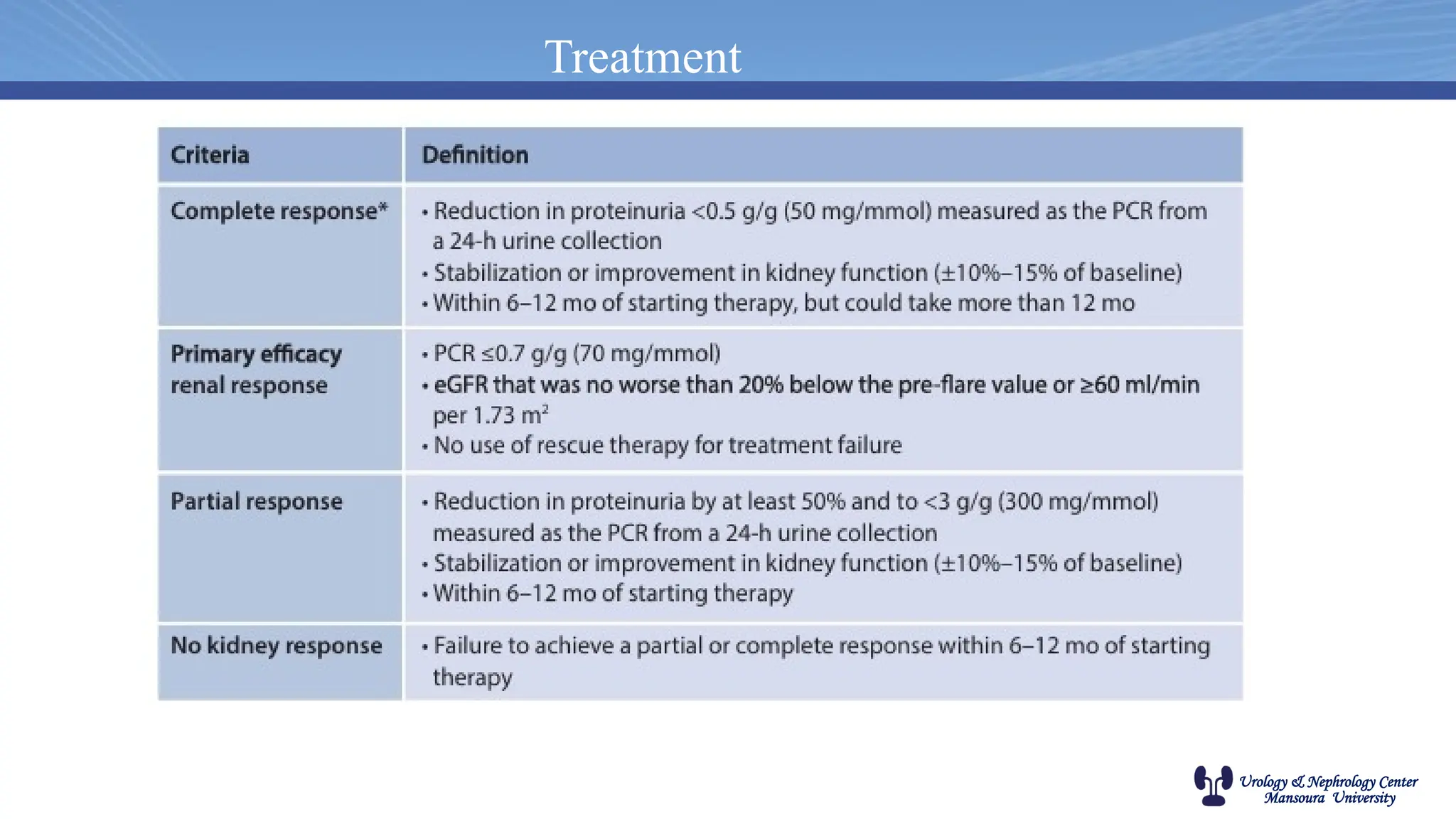
After 6 months of treatment, look for response
Responsive patients: Maintenance treatment for 2-3 years:
Oral prednisolone: ↓to 10 mg/day for further 6 months (± further tapering to 5-7.5 mg/day if remission is
maintained)
MMF: Continue on 2 gram/day
MMF intolerant or seeking for pregnancy: Shift to azathioprine 1.5 -2 gram/day
MMF and azathioprine intolerant: Cyclosporine or tacrolimus
Relapsing patients
Mild relapse: Resume maintenance therapy on which the patient was in remission
Moderate-severe relapse: Repeat induction therapy (2nd cyclophosphamide course is only allowed after
group discussion)
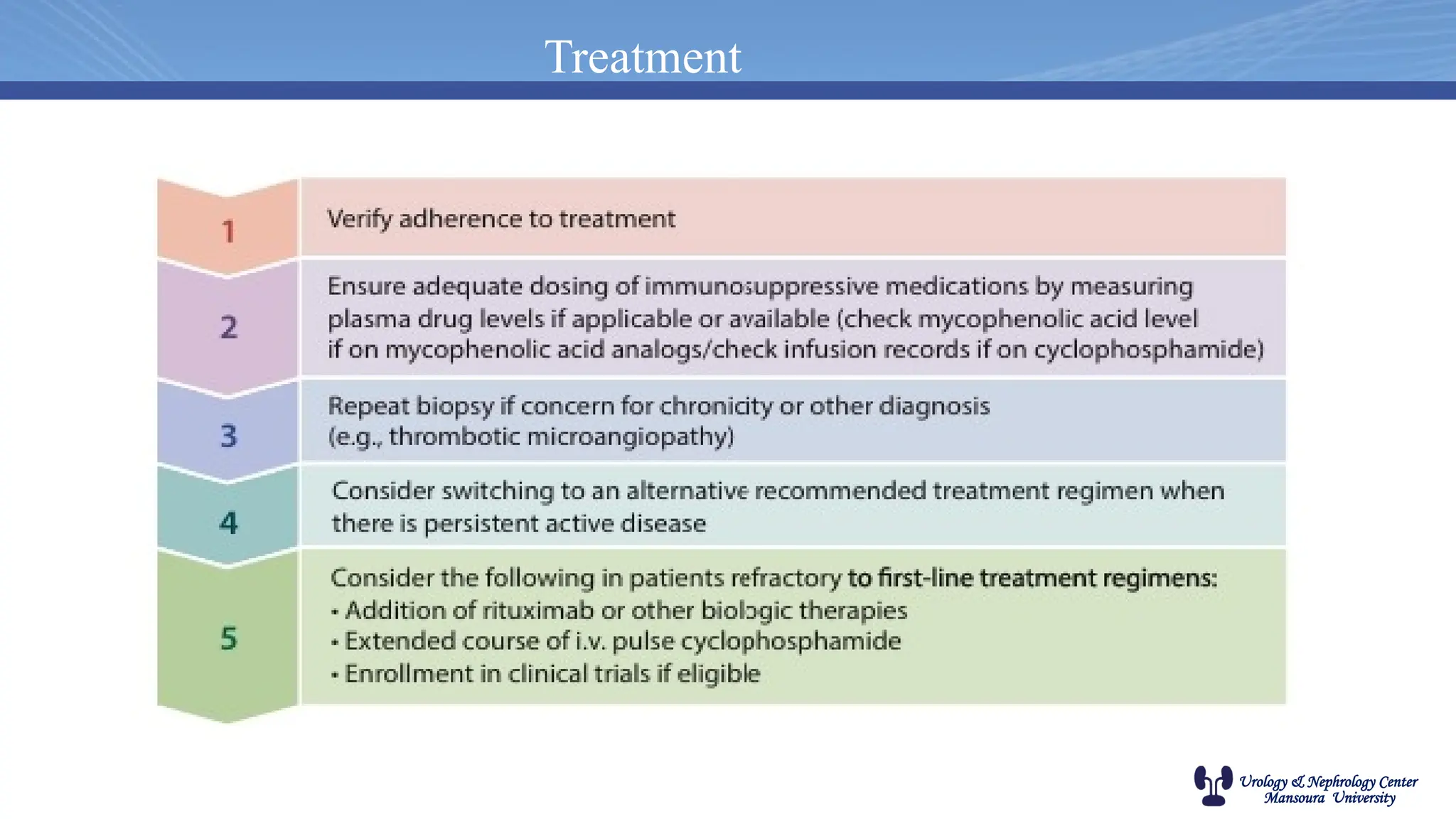
Resistant patients
Resistance to either cyclophosphamide or MMF: Shift to the other drug
Cyclophosphamide and MMF resistance: Multi-target therapy (steroids+MMF+CNI)
Multi-target therapy-resistant cases: Group discussion ± rituximab ± plasma exchange
Urology & NephrologyCenter
Mansoura University
UNC protocol
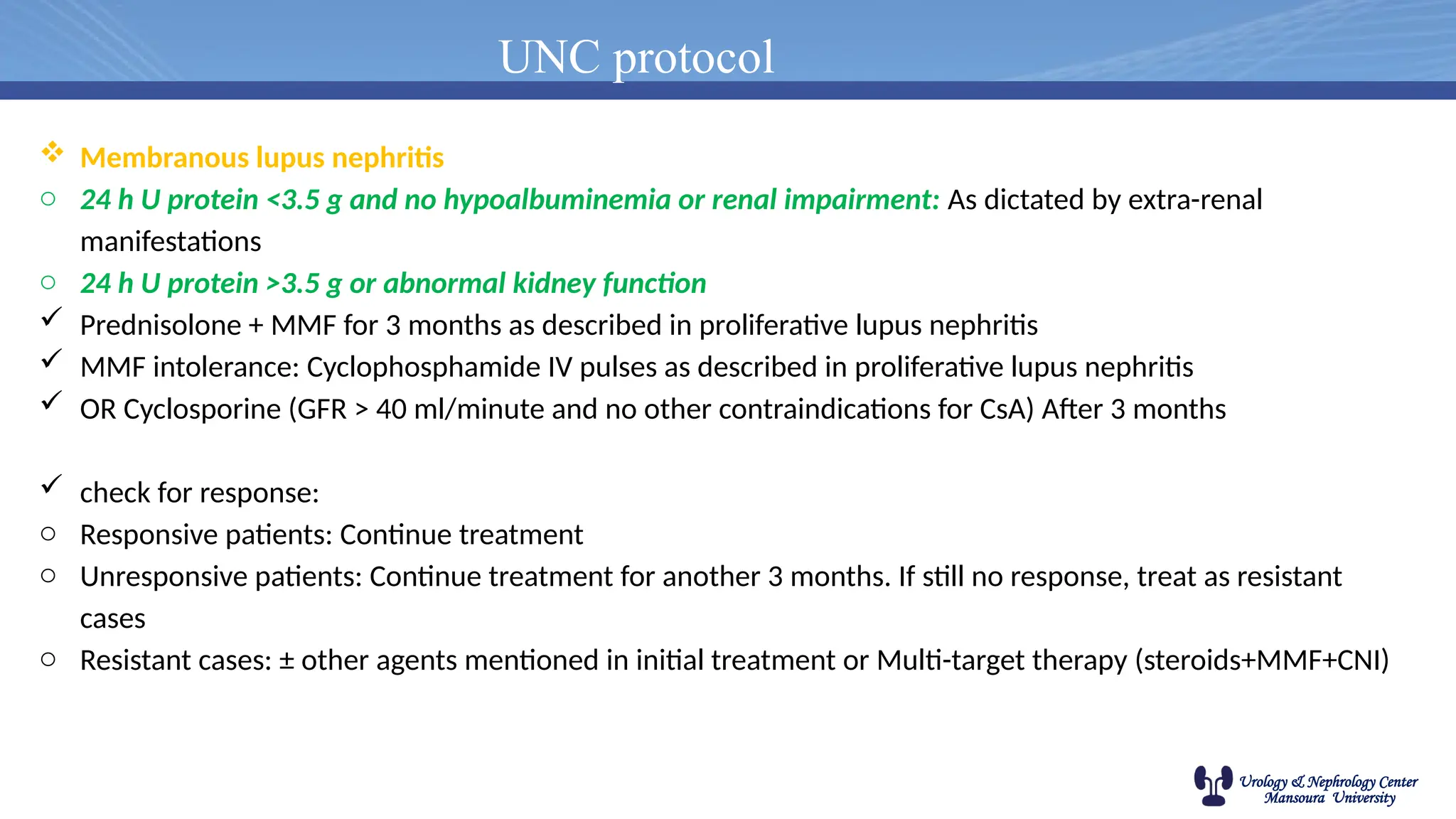
Membranous lupus nephritis
o 24 h U protein <3.5 g and no hypoalbuminemia or renal impairment: As dictated by extra-renal
manifestations
o 24 h U protein >3.5 g or abnormal kidney function
Prednisolone + MMF for 3 months as described in proliferative lupus nephritis
MMF intolerance: Cyclophosphamide IV pulses as described in proliferative lupus nephritis
OR Cyclosporine (GFR > 40 ml/minute and no other contraindications for CsA) After 3 months
check for response:
o Responsive patients: Continue treatment
o Unresponsive patients: Continue treatment for another 3 months. If still no response, treat as resistant
cases
o Resistant cases: ± other agents mentioned in initial treatment or Multi-target therapy (steroids+MMF+CNI)
40.
Urology & NephrologyCenter
Mansoura University
UNC protocol
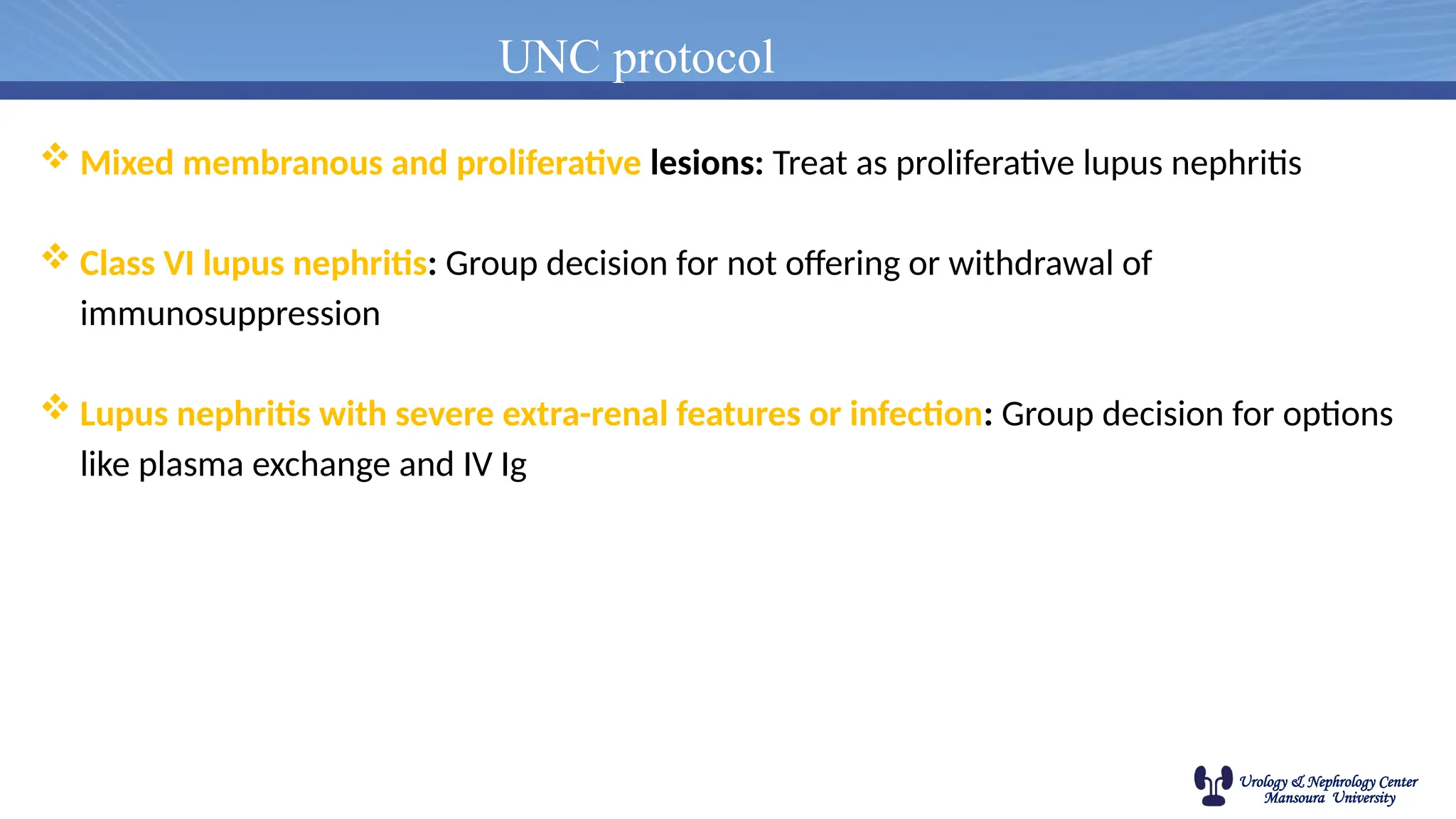
Mixed membranous and proliferative lesions: Treat as proliferative lupus nephritis
Class VI lupus nephritis: Group decision for not offering or withdrawal of
immunosuppression
Lupus nephritis with severe extra-renal features or infection: Group decision for options
like plasma exchange and IV Ig
Urology & NephrologyCenter
Mansoura University
LN and transplantation
• The risk of recurrence is much lower (2- 9%) if compared with other glomerular
diseases.
• Thrombophilia screen is recommended in renal transplant candidates with SLE.
• Anticoagulation is indicated in recipients with antiphospholipid antibodies.
46.
Urology & NephrologyCenter
Mansoura University
• Risk factors for recurrent LN
1. Female gender
2. Younger age (< 33 years)
3. African American ethnicity
4. Antiphospholipid autoantibodies
ÇELTİK et al, Nephrology 21 (2016) 601–607
47.
Urology & NephrologyCenter
Mansoura University
• New onset proteinuria or Rapid worsening of previously existing proteinuria glomerular
hematuria should directly lead to the suspicion of lupus nephritis in the allograft.
• Diagnosis of RLN is made by biopsy and histopathologic evaluation by light
microscopy, immunofluorescence and electron microscopy
• Measurement of serologic parameters, such as complement levels and titers of anti-
double stranded DNA antibodies is not helpful in establishing the diagnosis in the
allograft.
Diagnosis of RLN
48.
Urology & NephrologyCenter
Mansoura University
• The existing immunosuppressive regimen to be modified.
• Depending on the clinical picture and morphologic lesions, we use either:
1. Higher doses of mycophenolate mofetil or (2-3 g/d)
2. initiate cyclophosphamide intravenously along with discontinuation of the
current antimetabolite.
3. Pulses of methylprednisolone, 500-1000 mg/d for 3 consecutive days,
which are followed by a tapering steroid regimen.
4. In cases of resistant RLN despite the use of mycophenolate mofetil and
cyclophosphamide, the only treatment option is rituximab along with an
increase in glucocorticoids.
Treatment of RLN
Urology & NephrologyCenter
Mansoura University
Case 1
• A 21-year-old woman was diagnosed with SLE 1 year ago. At that time, urine sediment was unremarkable,
serum creatinine was 0.6 mg/dL, and she had no proteinuria. She was treated with low-dose glucocorticoids and
hydroxychloroquine, with resolution of her symptoms. Over the past month, she noticed foamy urine and mild
ankle swelling. Evaluation showed blood on her urine dipstick, 24-hour urine with 4 g protein, serum creatinine
of 1 mg/dL, and a rising dsDNA titer with both C3 and C4 now newly decreased. A kidney biopsy revealed
class IV LN, without crescents or glomerular capillary necrosis. The patient wants children in the future.
Considering options for initial therapy for this patient’s LN, which of the following statements is incorrect?
A. She could be treated with MMF and glucocorticoids.
B. She could be treated with a calcineurin inhibitor in combination with MMF and glucocorticoids.
C. She could be treated with low-dose cyclophosphamide and receive ovarian protection.
D. She could be treated with belimumab alone.
51.
Urology & NephrologyCenter
Mansoura University
Case 2
• A 24-year-old woman has been treated for the last 6 months with MMF 3 g/day and a tapering dose of
glucocorticoids for active focal proliferative class III LN. Her initial proteinuria decreased from 3.4 g/day to
1.2 g/day, urine sediment became inactive, serum creatinine decreased from 1.6 to 0.9 mg/dL over the 6
months of therapy, anti-dsDNA titer declined, and serum complement values returned to normal. She has
tolerated her treatment well and reports no side effects. What should be done with her immunosuppression?
A. Continue the current dose of MMF, follow patient for a complete renal remission, and when achieved,
reduce MMF to 2 g/ day and continue for at least 36 months of total immunosuppressive therapy, with
ongoing monitoring for any evidence of LN relapse.
B. Change to intravenous cyclophosphamide at 500 mg every 2 weeks for 6 doses and then administer
azathioprine at 2 mg/kg daily.
C. Add a calcineurin inhibitor to her current regimen.
D. Add rituximab to her current regimen.
52.
Urology & NephrologyCenter
Mansoura University
Case 3
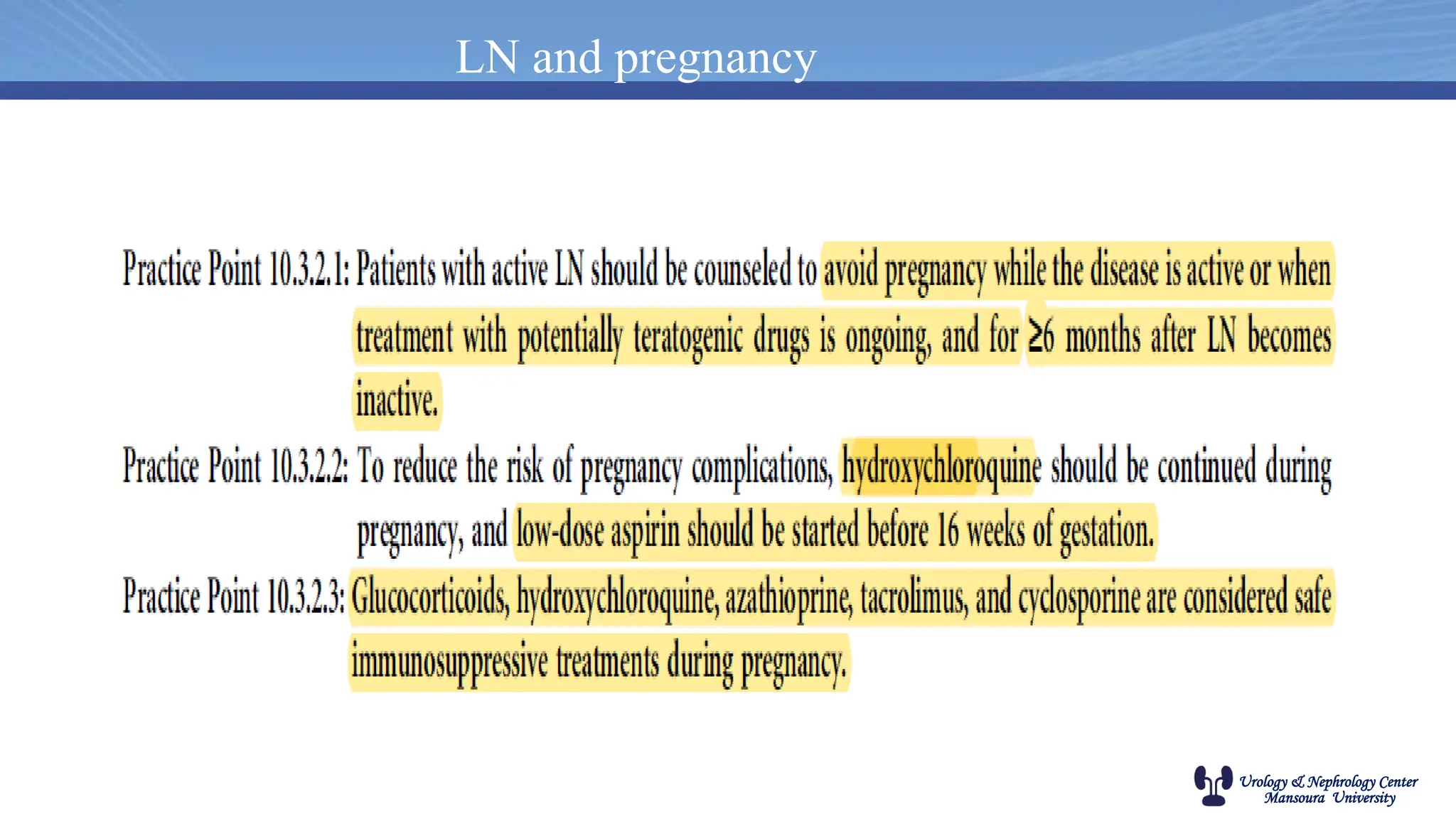
• A 32-year-old woman with a past history of LN wants to become pregnant and is concerned
about flares during the pregnancy.
Which of the medications listed should NOT be used during pregnancy?
A. Glucocorticoids
B. Calcineurin inhibitor
C. Hydroxychloroquine
D. Azathioprine
E. Mycophenolate mofetil
53.
Urology & NephrologyCenter
Mansoura University
Case 4
• A 28-year-old man had been diagnosed 4 years ago with class IV LN by kidney biopsy. He was
treated with MMF and glucocorticoids, and his kidney function improved to an eGFR of 89 mL/
min/1.73 m2. Proteinuria fell from 2.7 g/day to 950 mg/day. His antidsDNA antibody titer fell by
75% and his C3 complement increased to the normal range, but C4 remained low. He has been on
MMF 2 g/day for 3 years. He has been on 5 mg of prednisone every other day for 2 years. He has
had no extrarenal signs or symptoms of lupus for over 3 years. He wants to know if he needs to
stay on immunosuppression or can safely come off. What should be done?
A. Continue his MMF and prednisone until the anti-dsDNA antibody is no longer detectable
and then stop immunosuppression.
B. Order a kidney biopsy to determine whether there is any residual histologic activity.
C. Continue his MMF and prednisone until his C4 level is in the normal range and then stop
immunosuppression.
D. Continue his MMF and prednisone until his proteinuria is less than 250 mg/day.
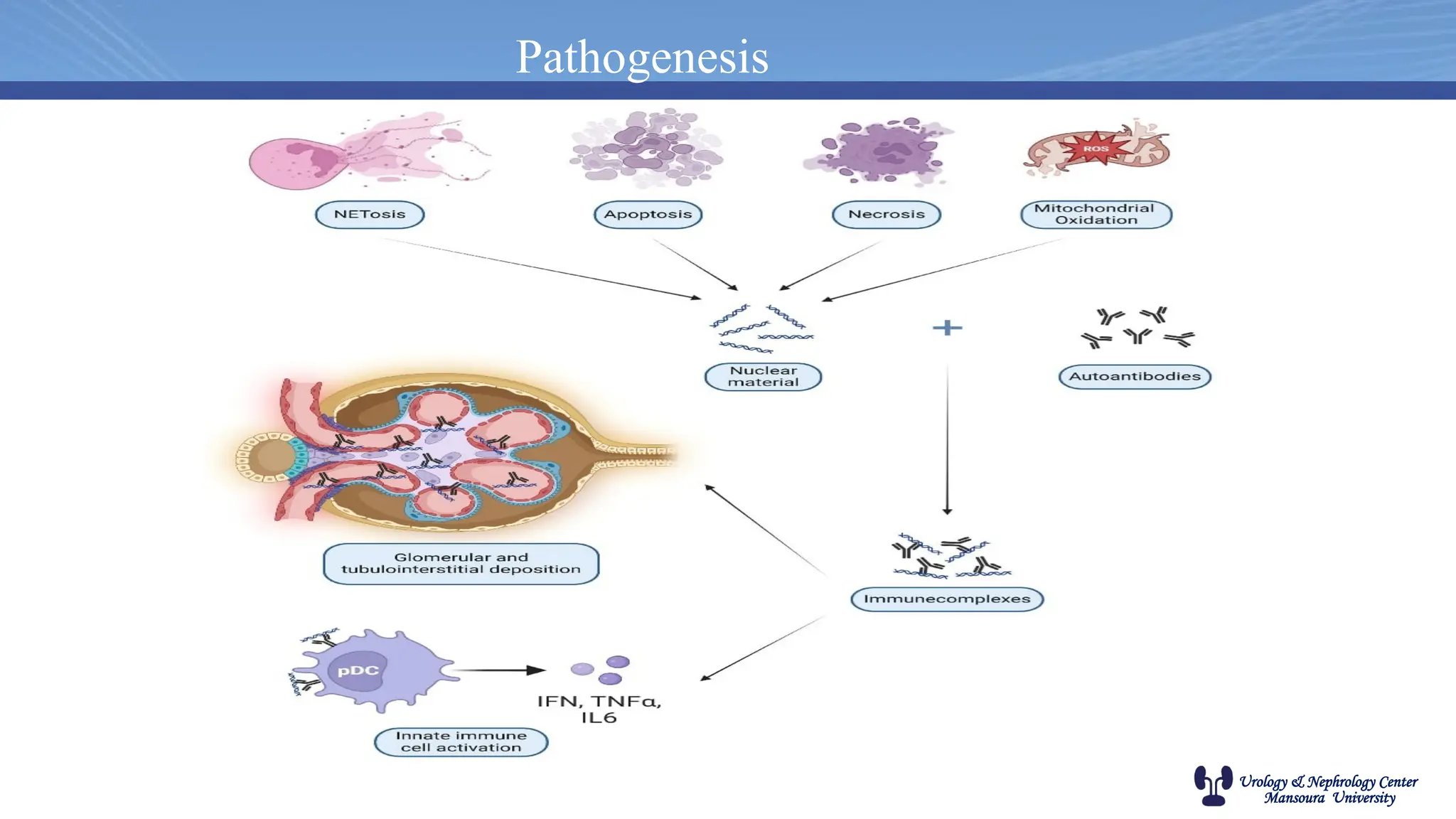
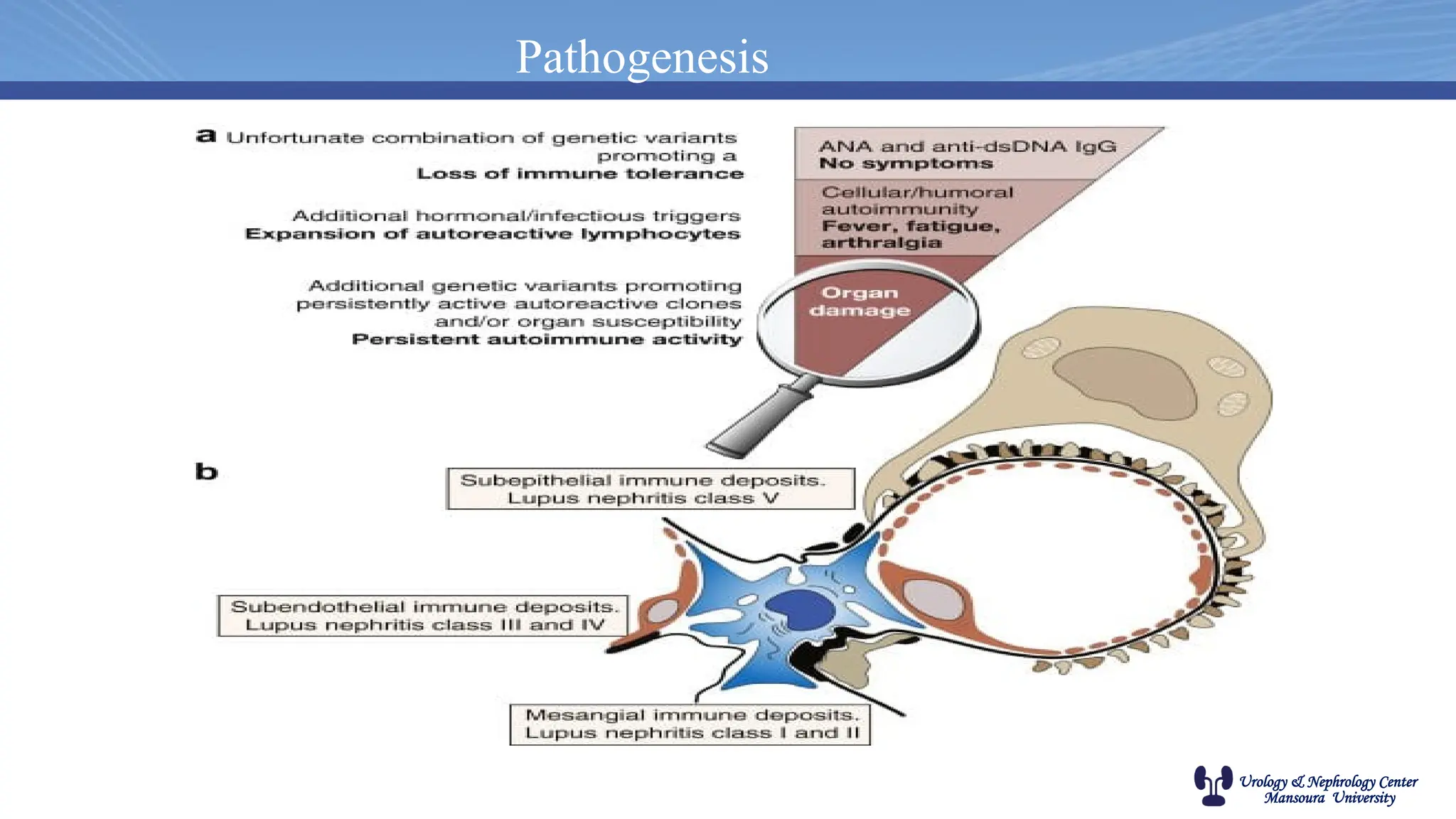
#8 Early in disease, clearance of apoptotic cells is impaired and nuclear autoantigens released from these cells stimulate expression of interferon-α
(IFN-α), which facilitates the generation of antigen-presenting cells, promotes the differentiation of autoreactive B cells into plasma cells, and fosters the development of T helper cells.