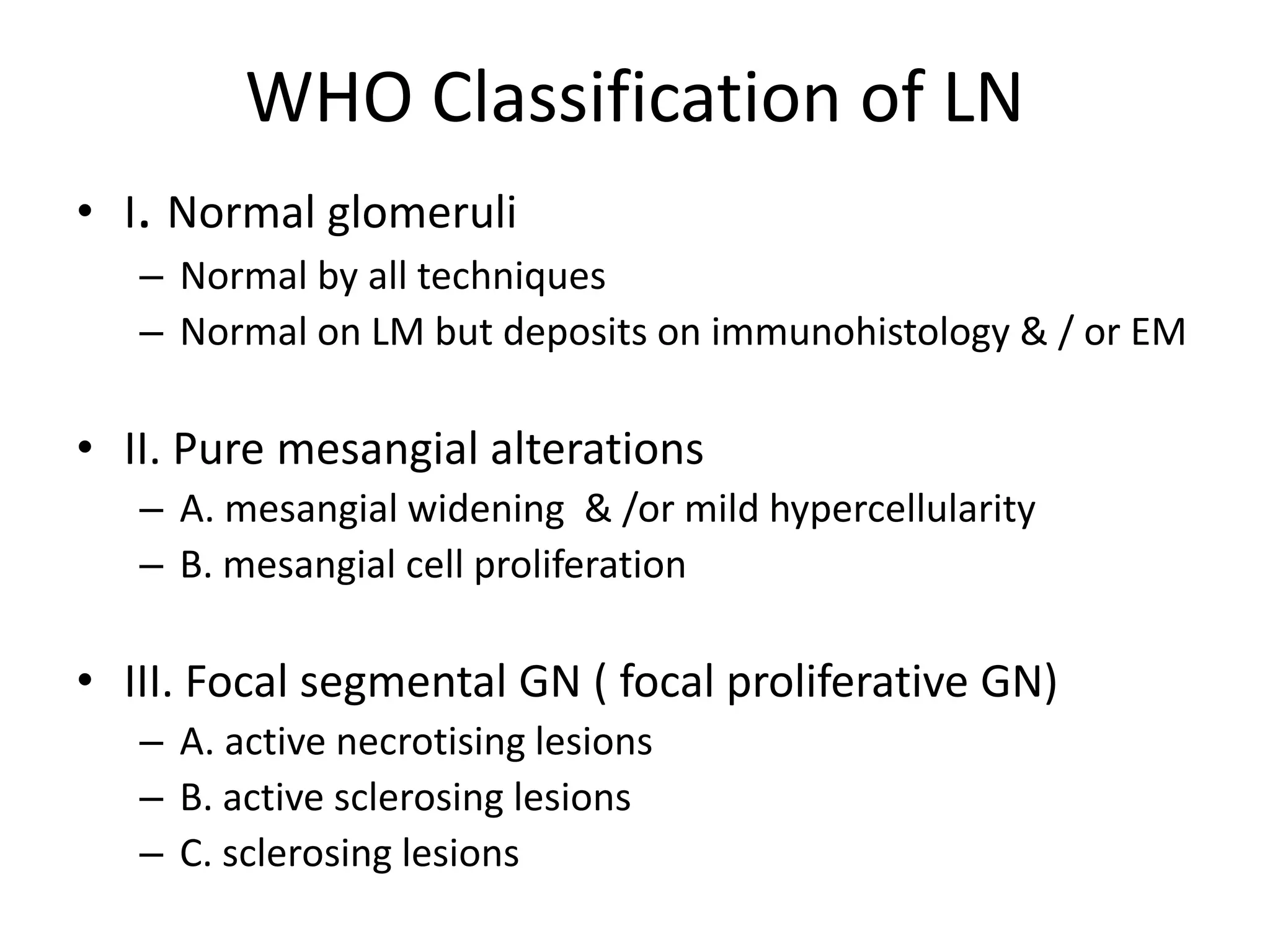
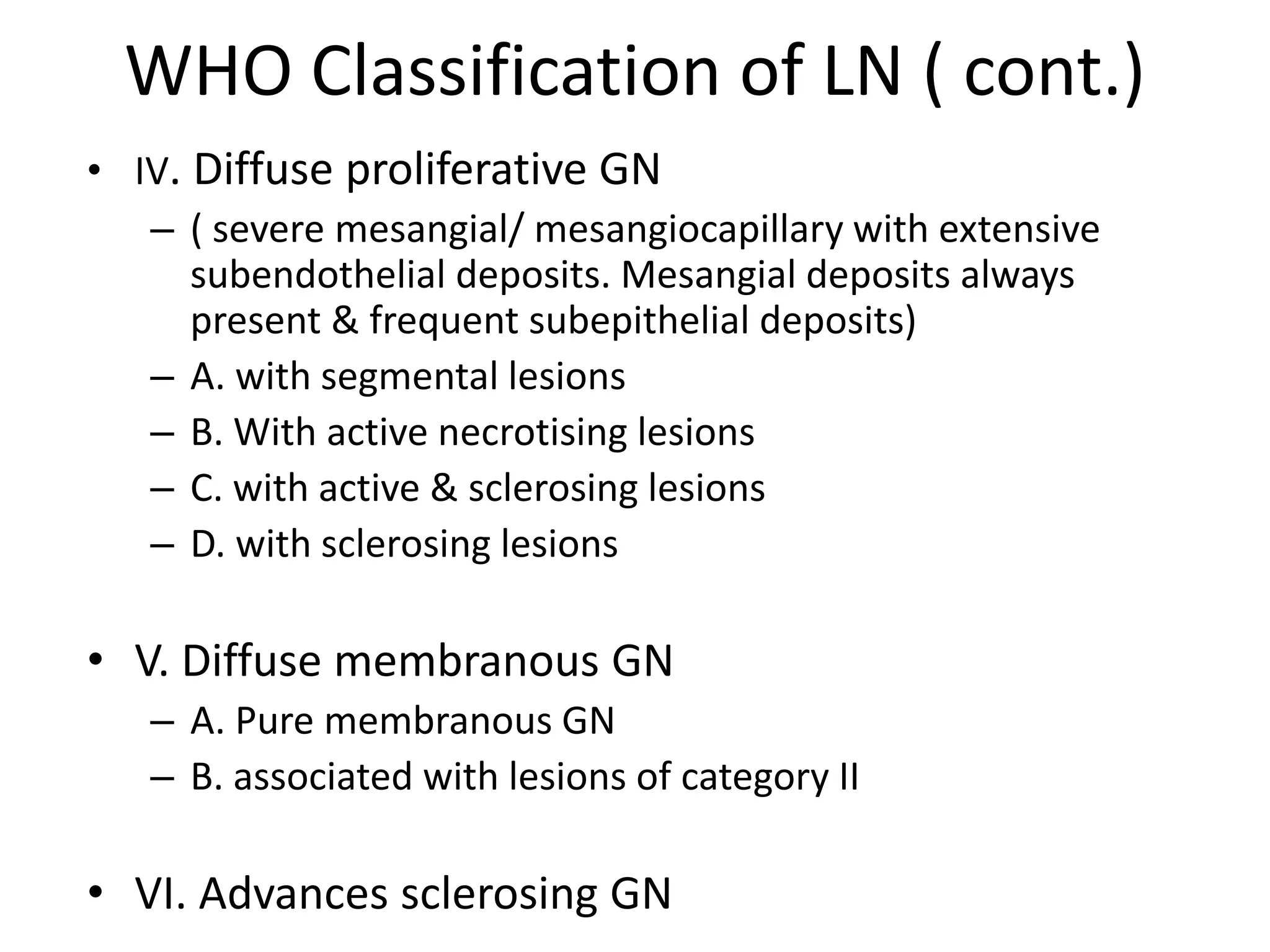
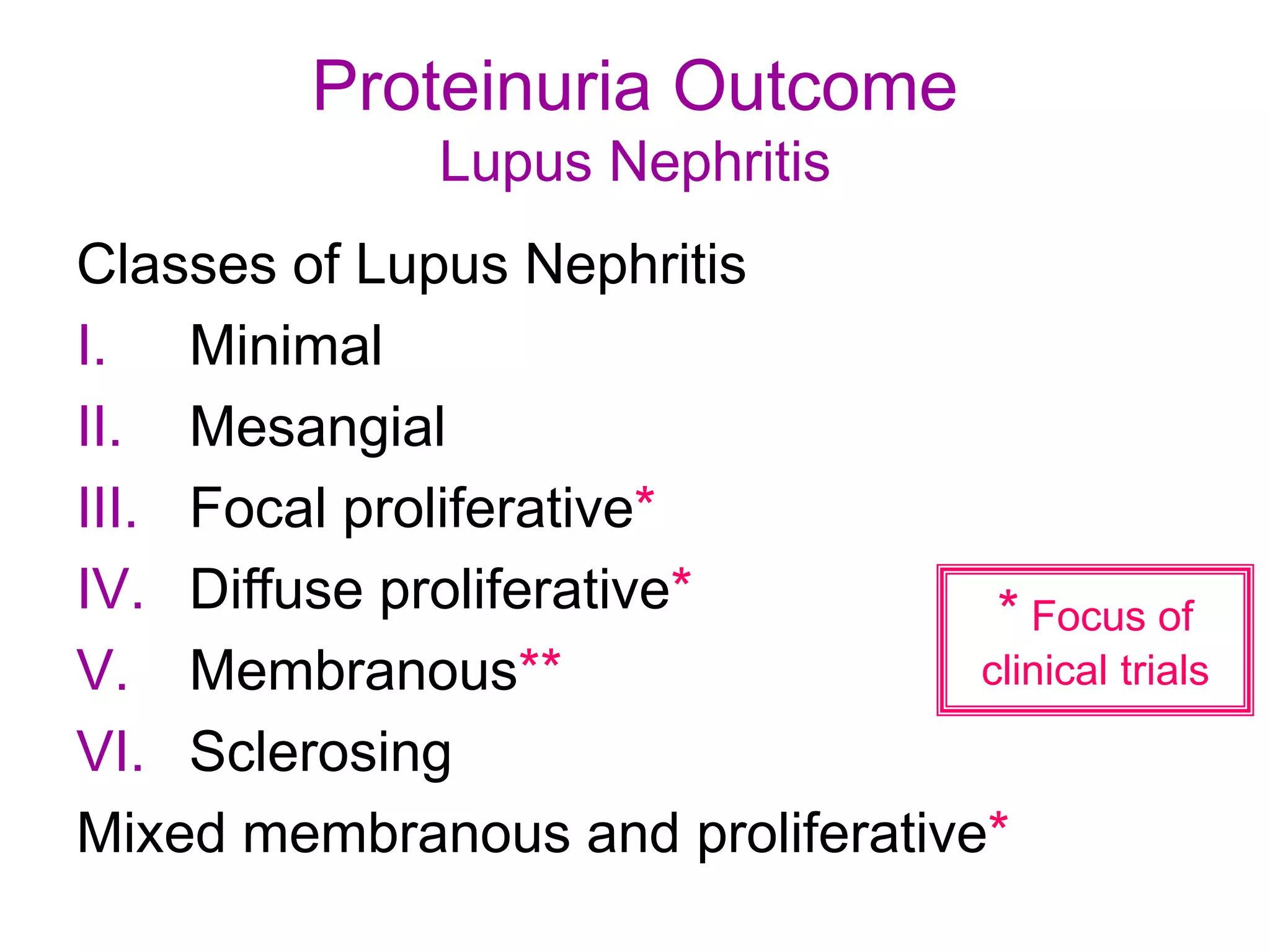
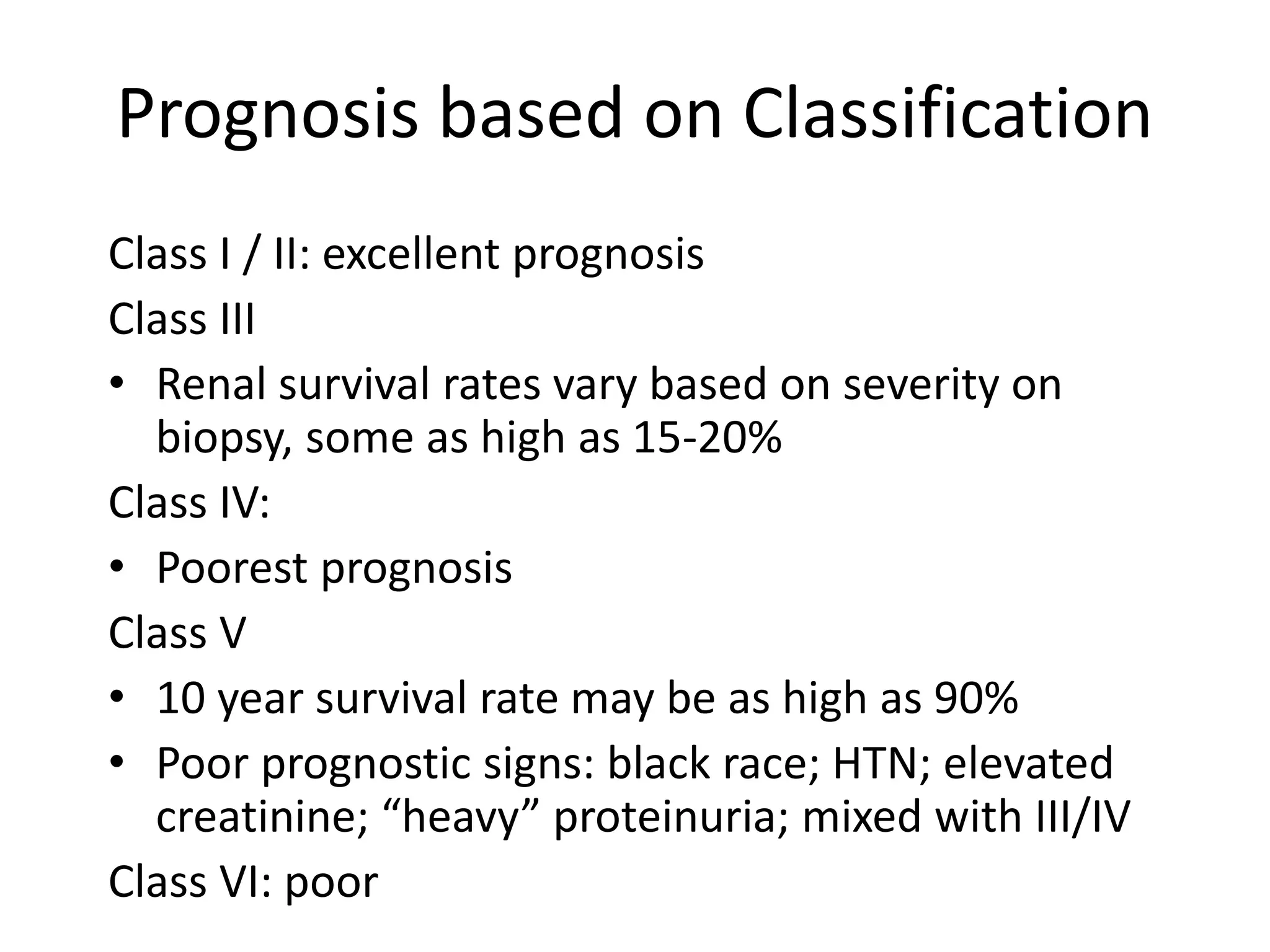
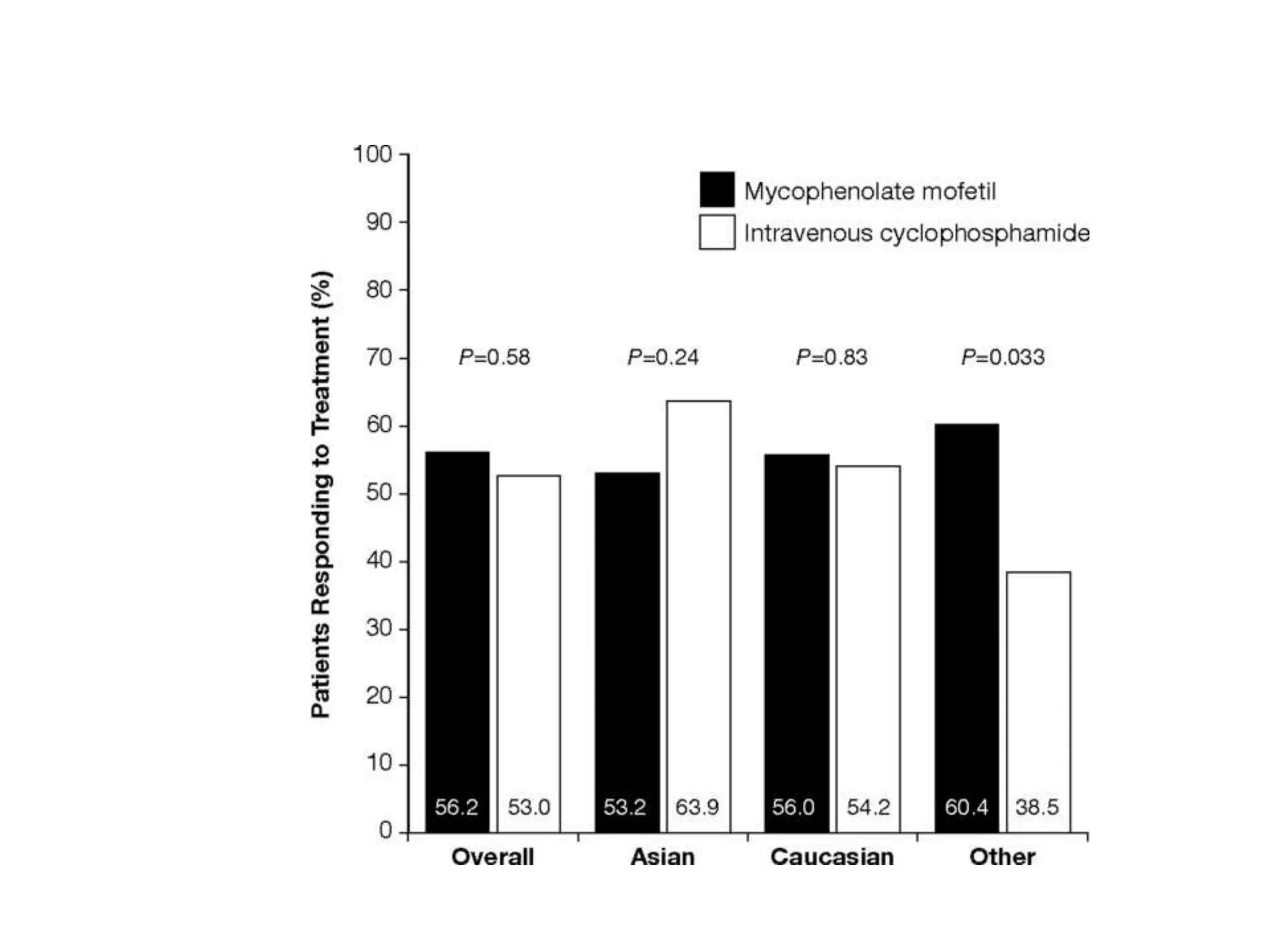
This document discusses recent treatment trials for lupus nephritis and provides an example of a patient case. It defines classifications of glomerular pathology and reviews a kidney biopsy specimen. It covers the pathogenesis of lupus nephritis including the role of immune complexes and antibodies. Treatment considerations are outlined for induction therapy with cyclophosphamide or mycophenolate mofetil and maintenance therapy with azathioprine. Clinical trials comparing various regimens are summarized.