Downloaded 28 times

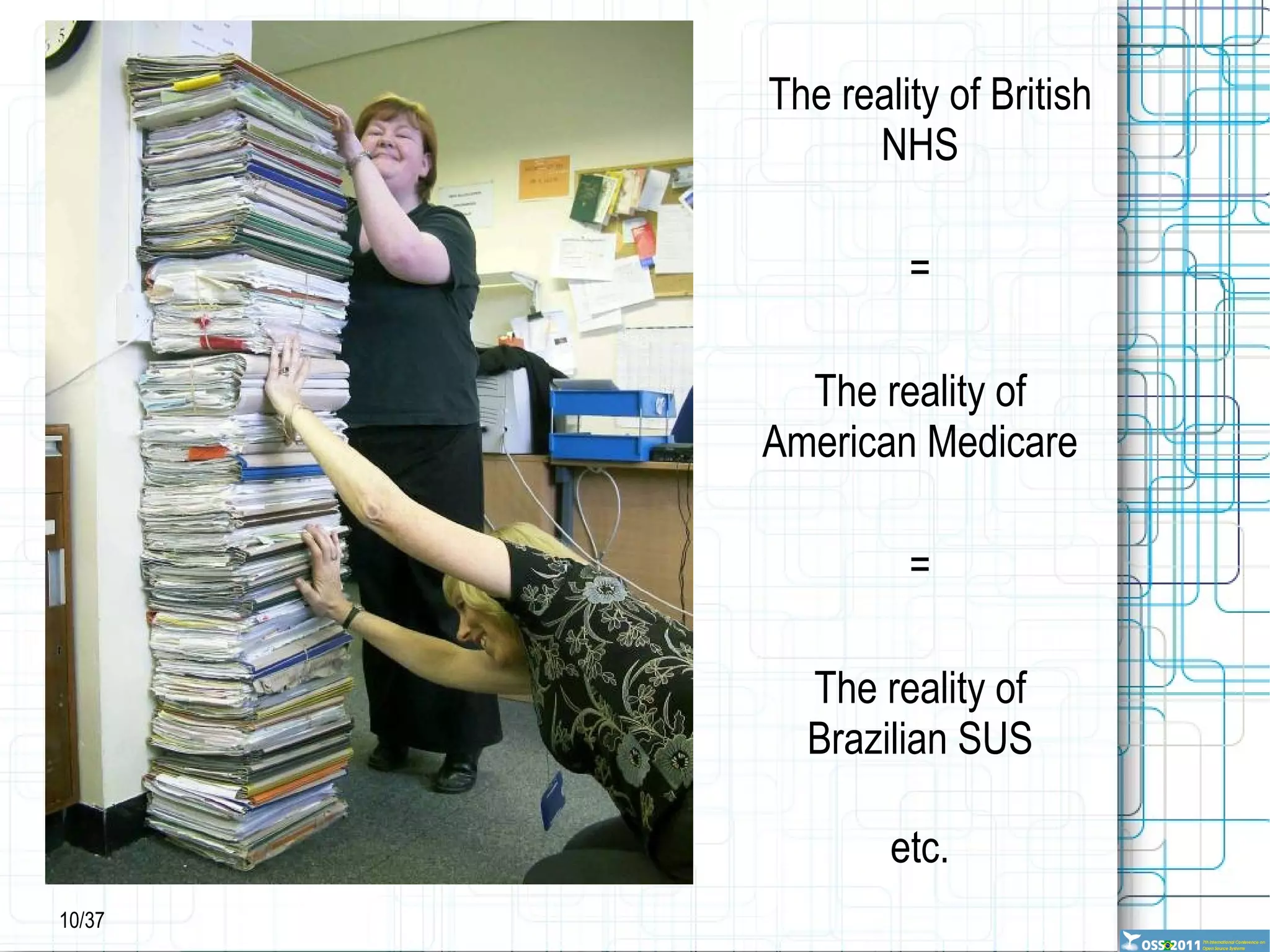
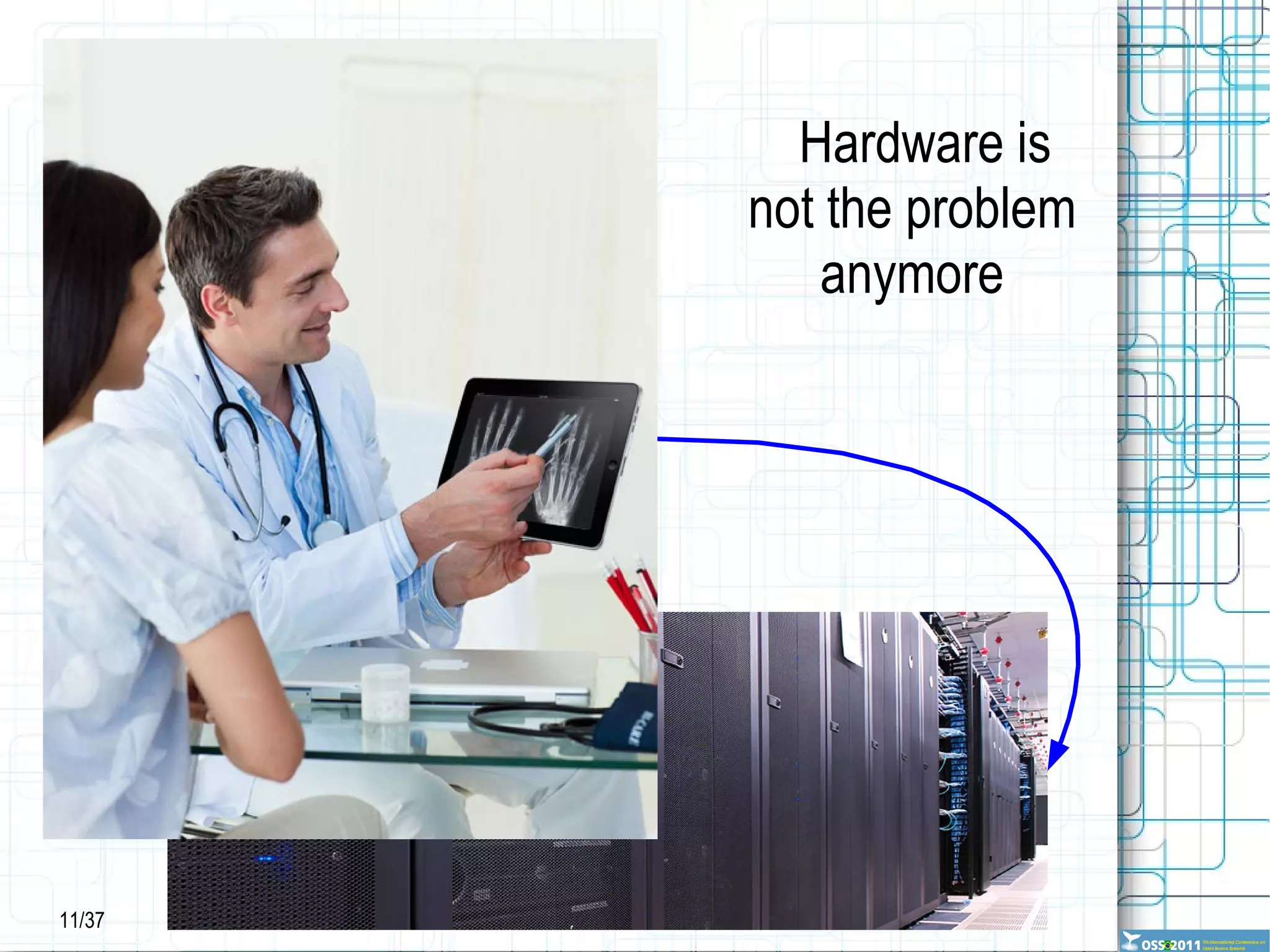
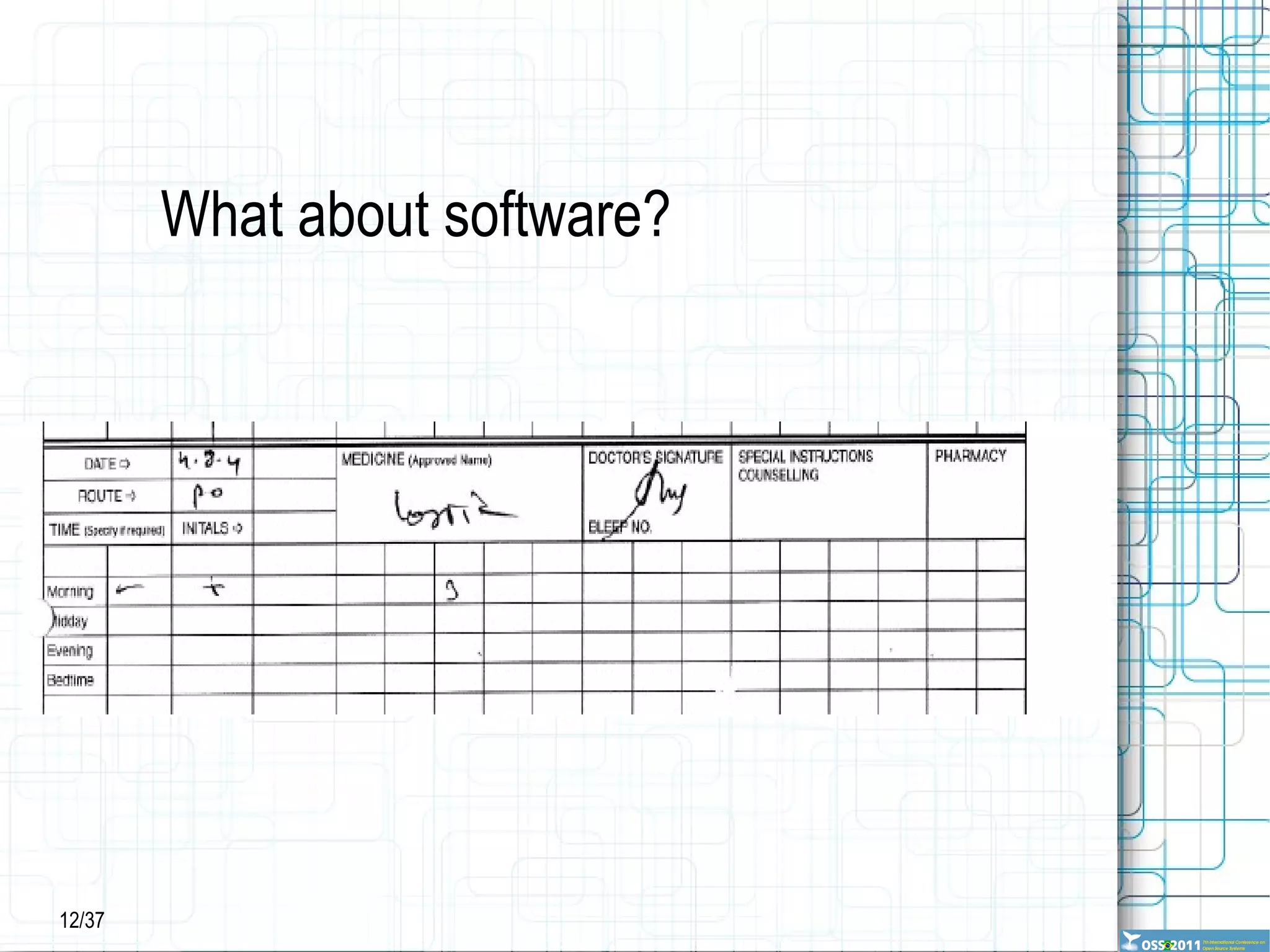
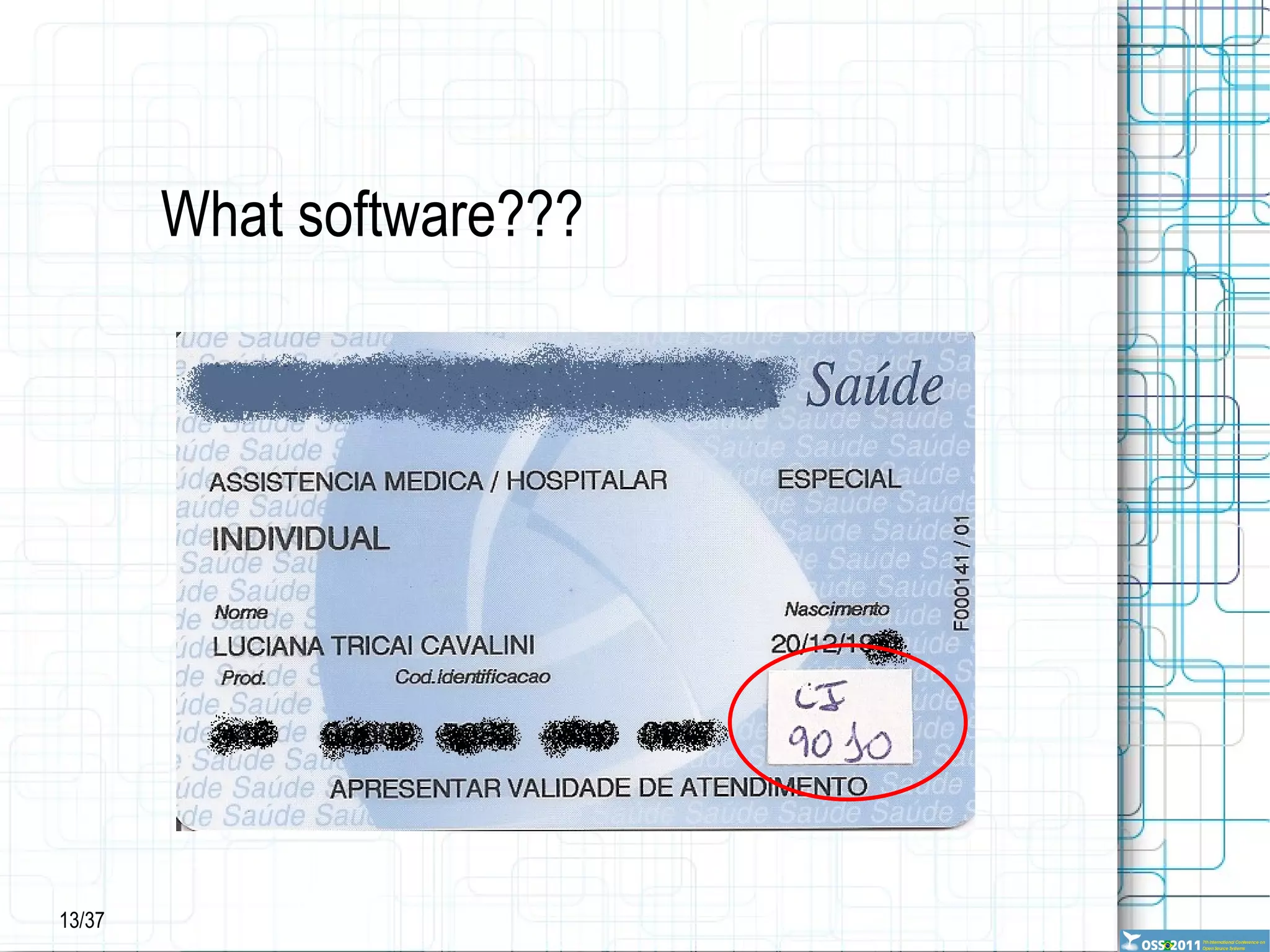
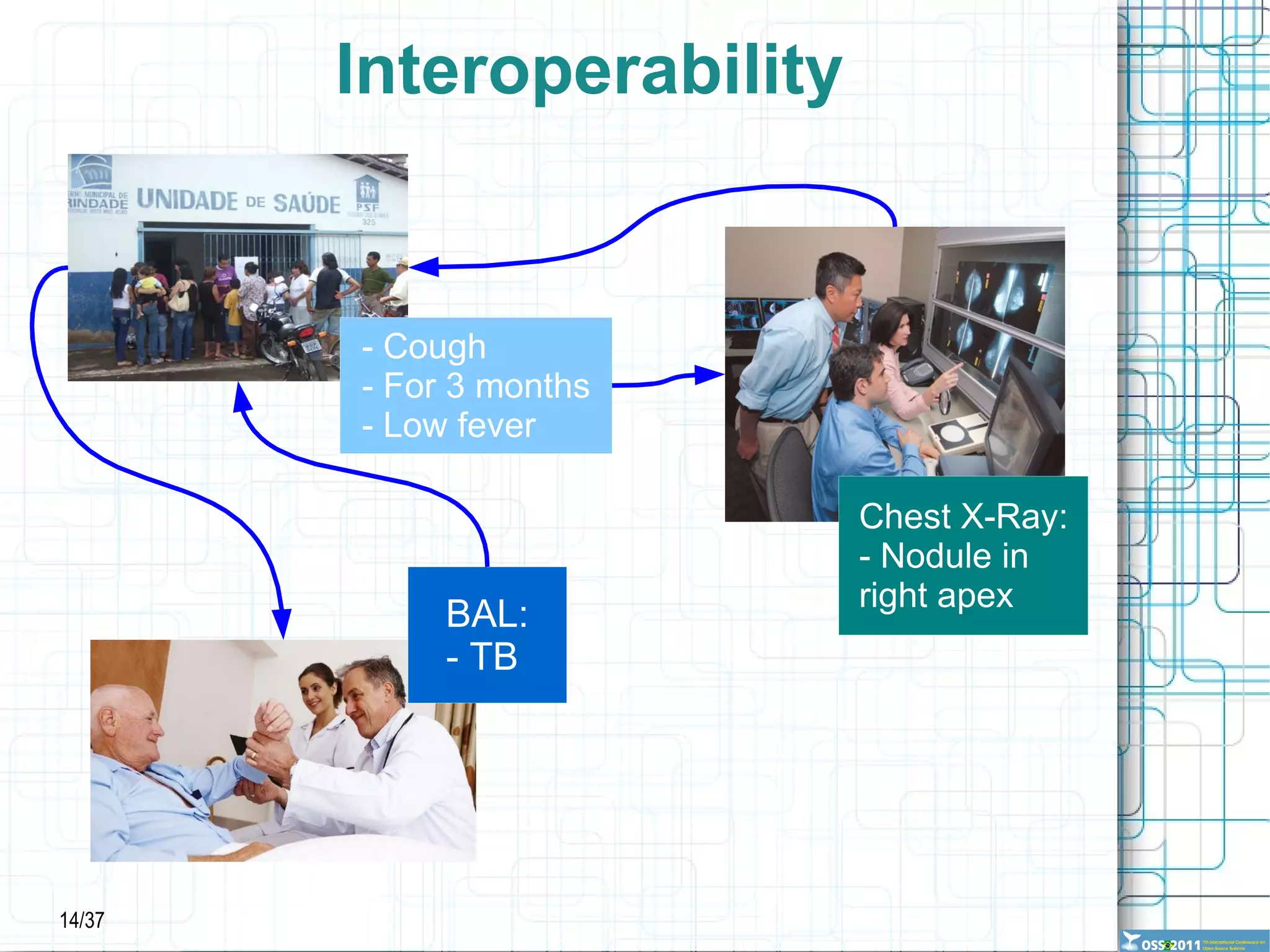
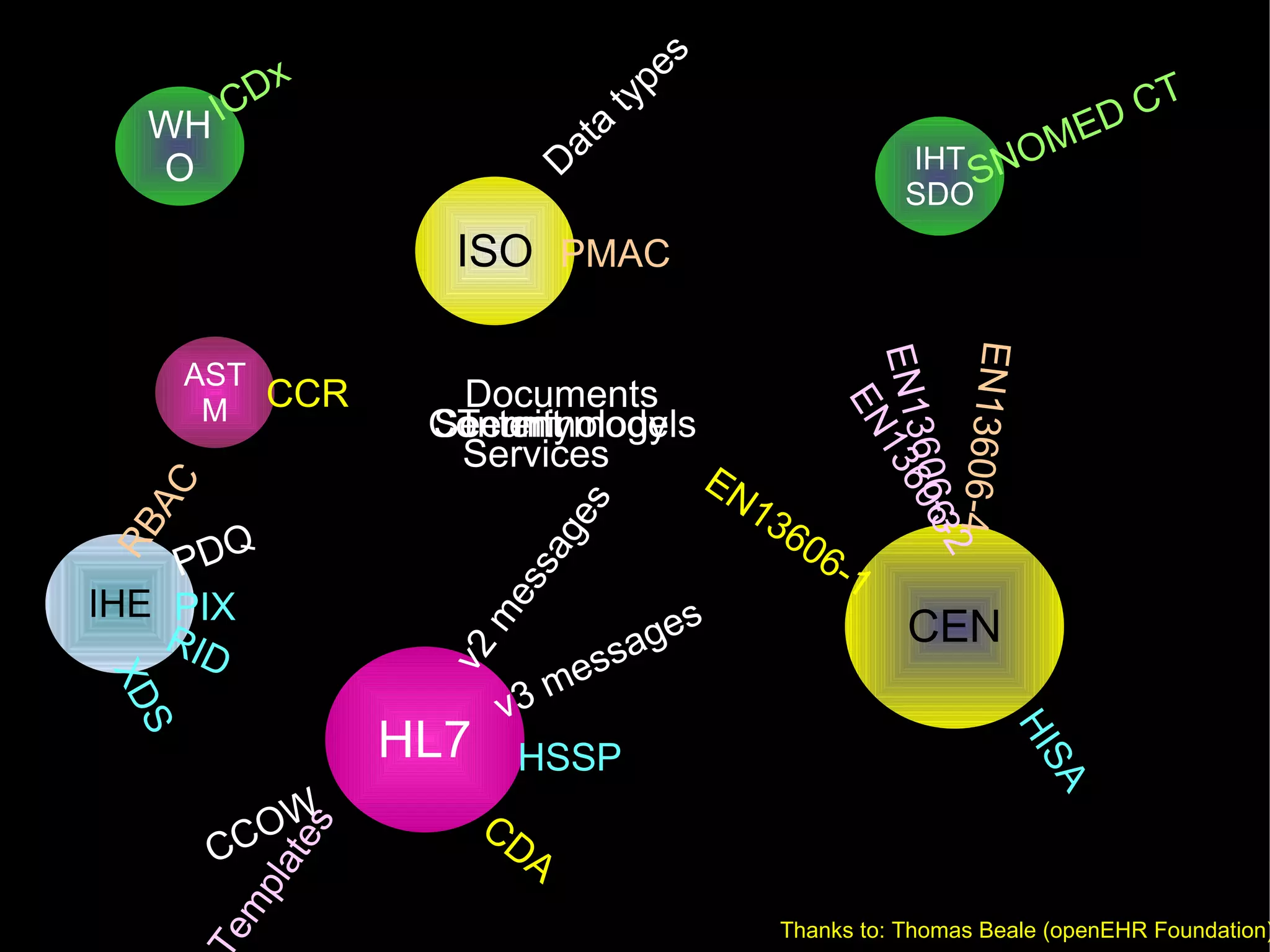
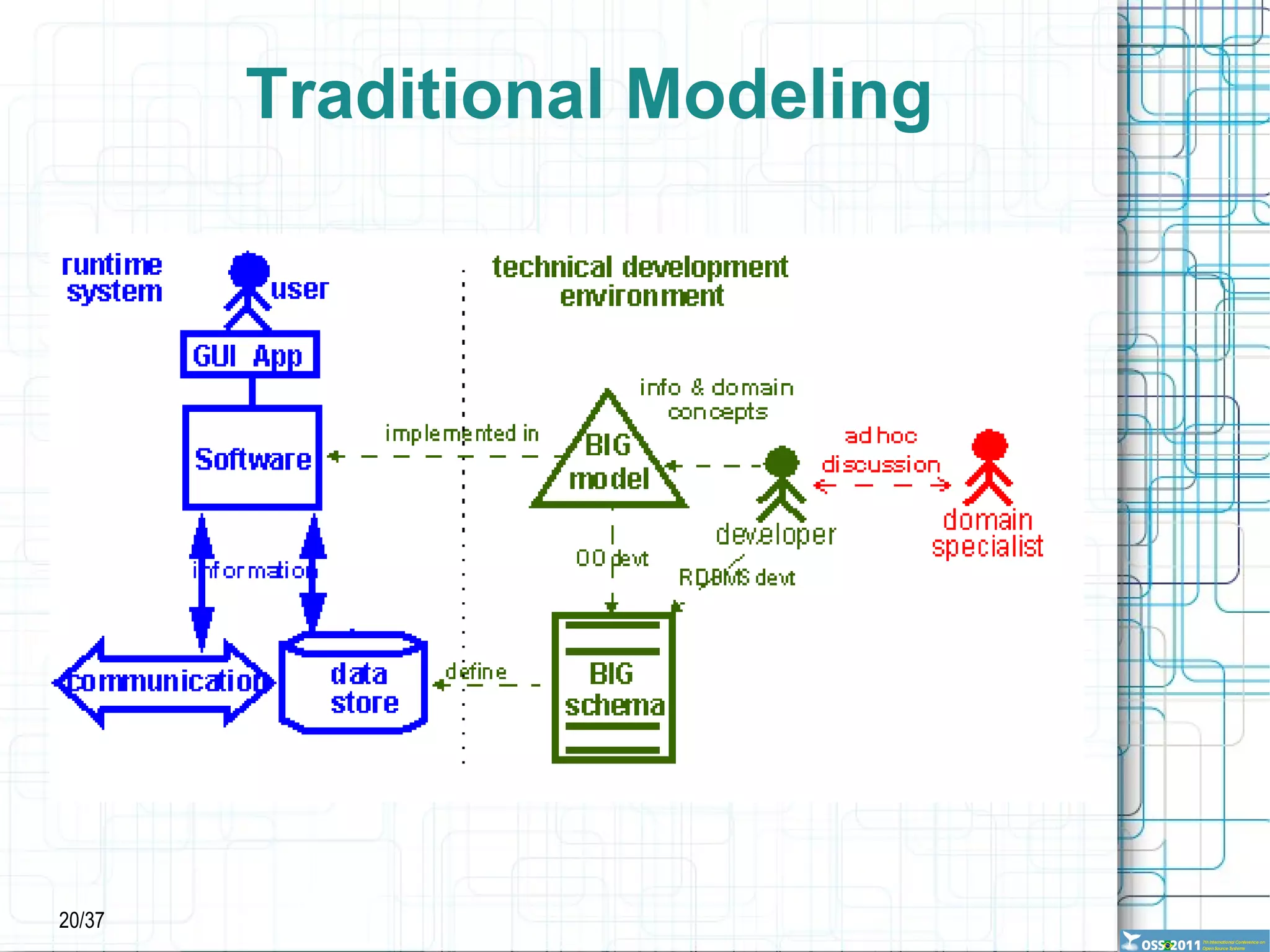
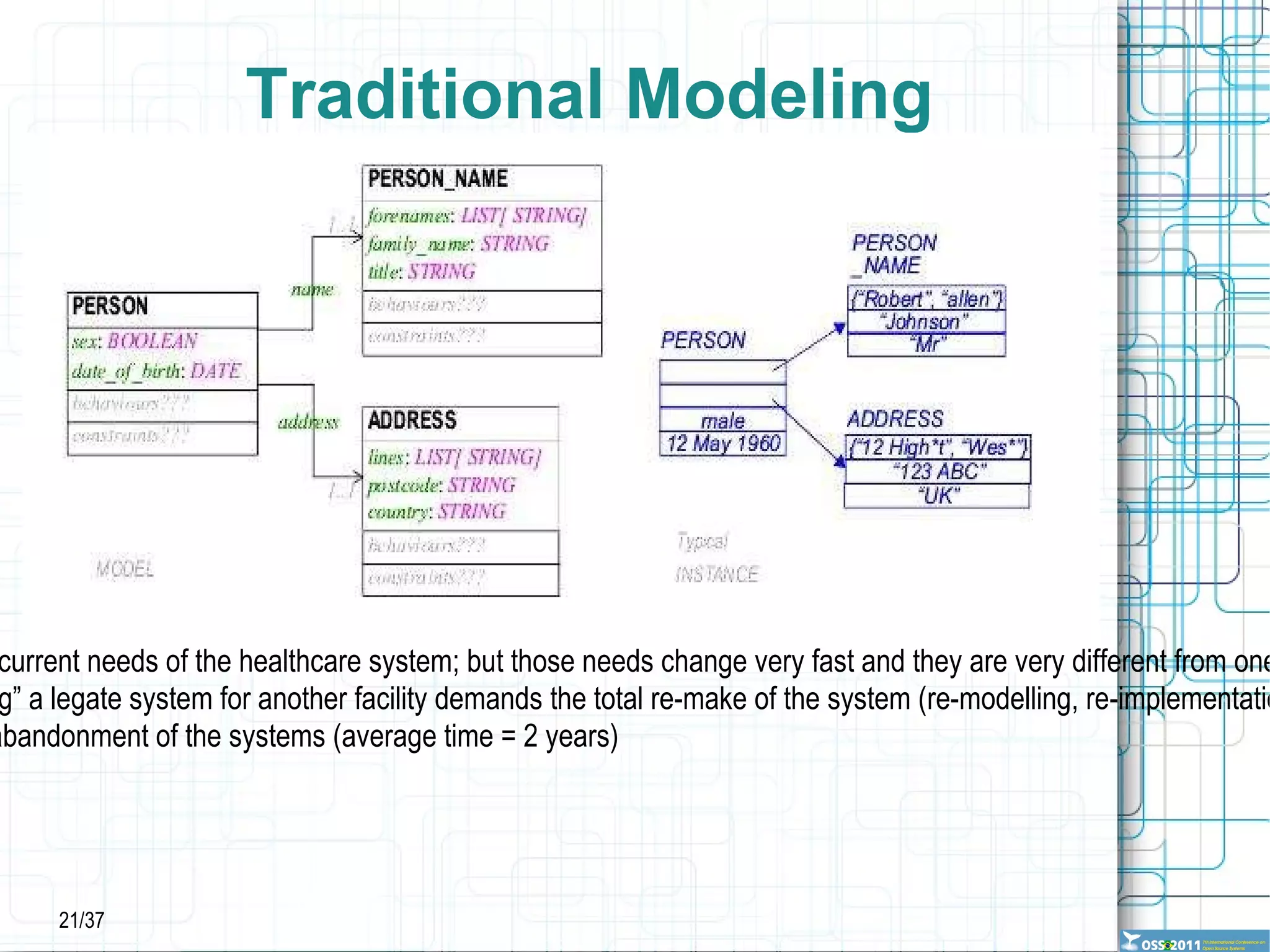
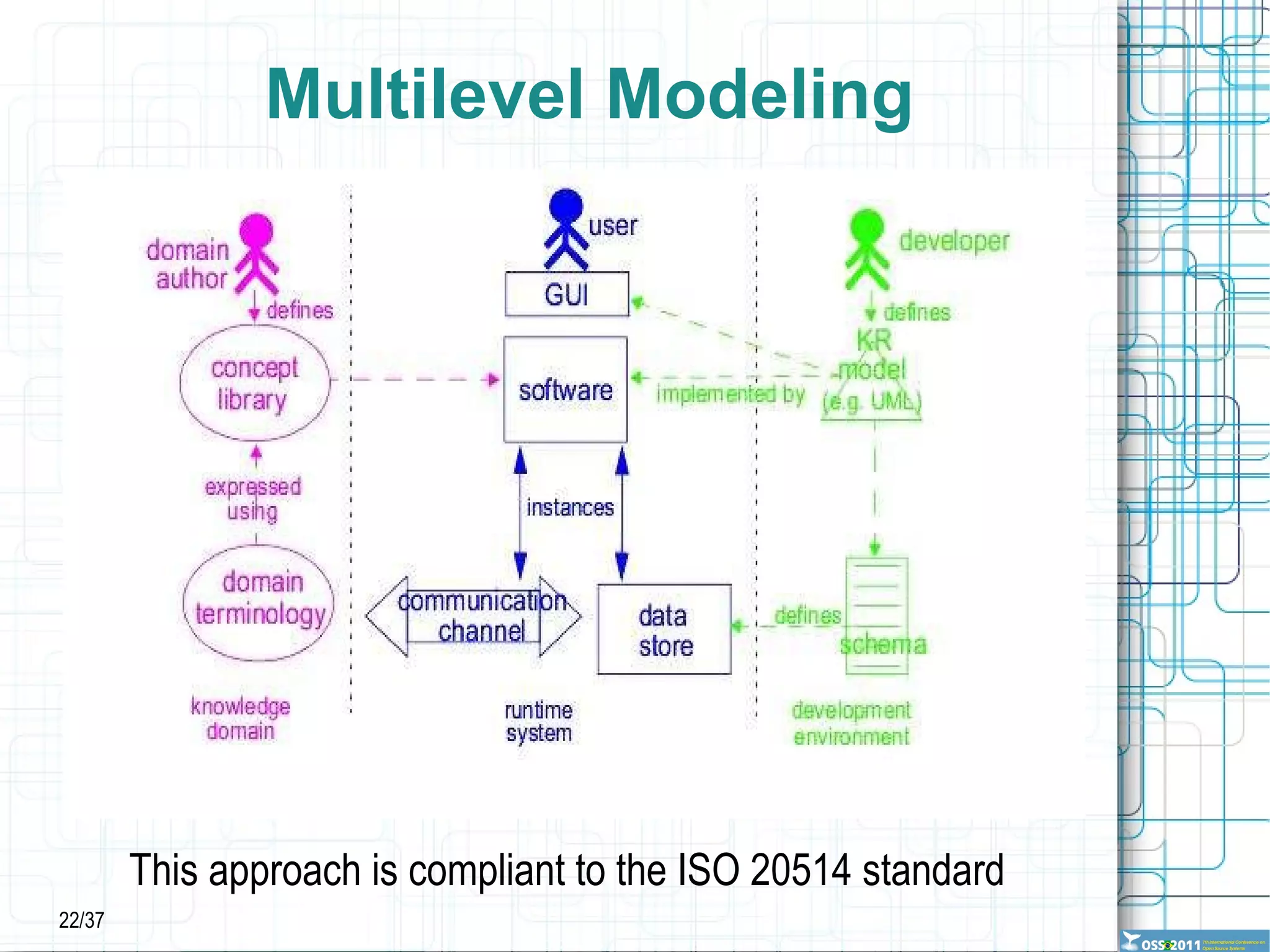

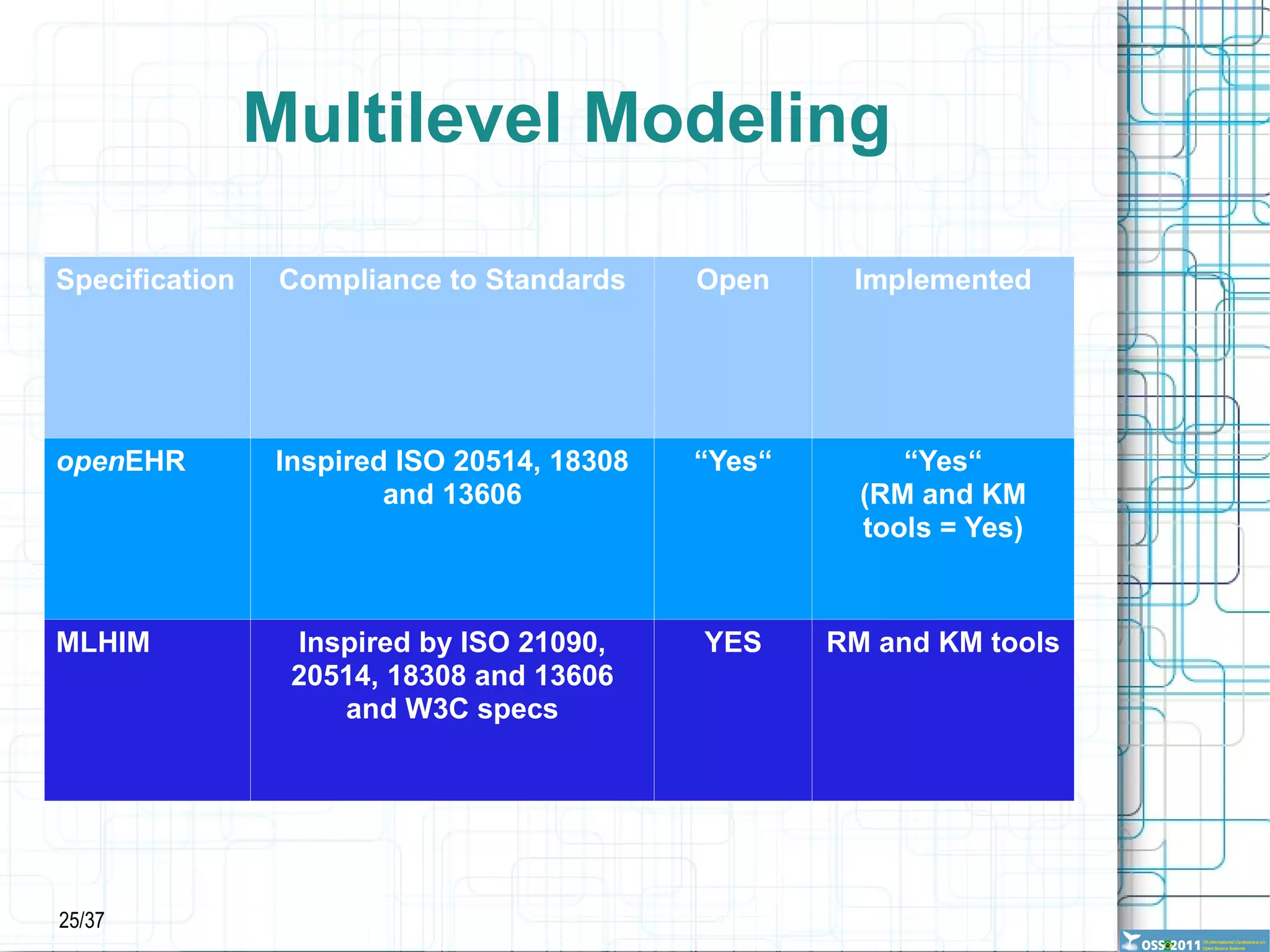
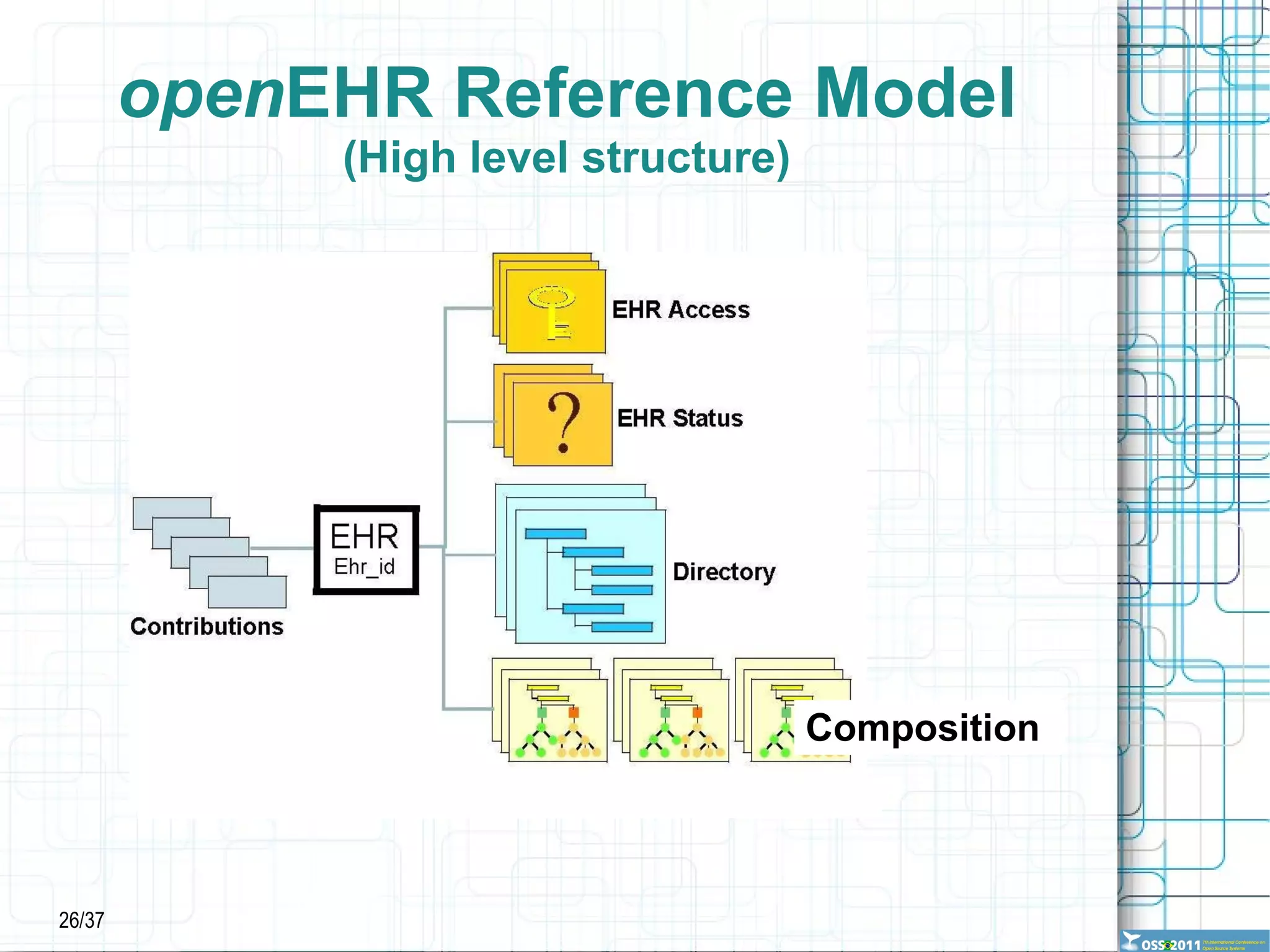
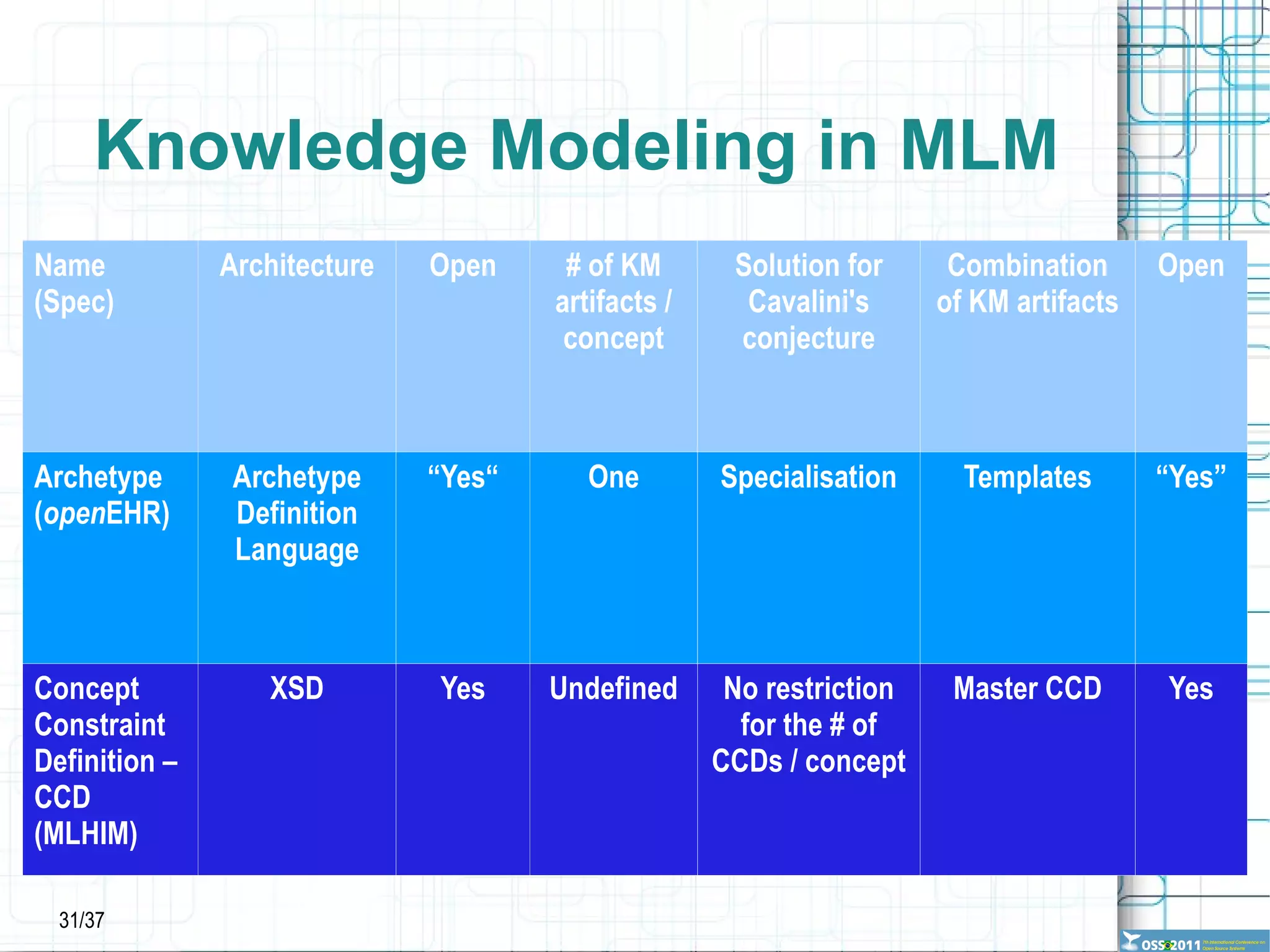
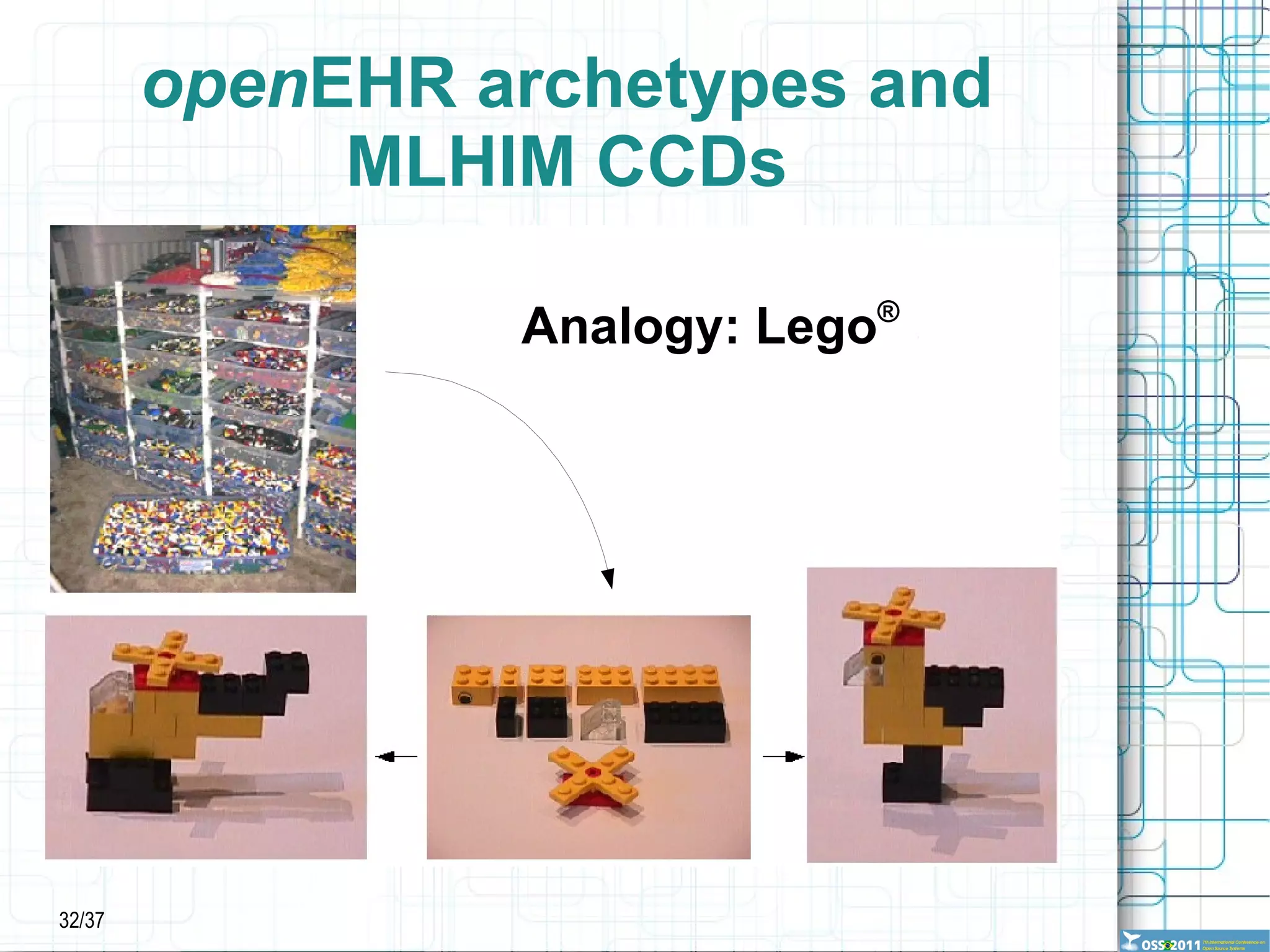
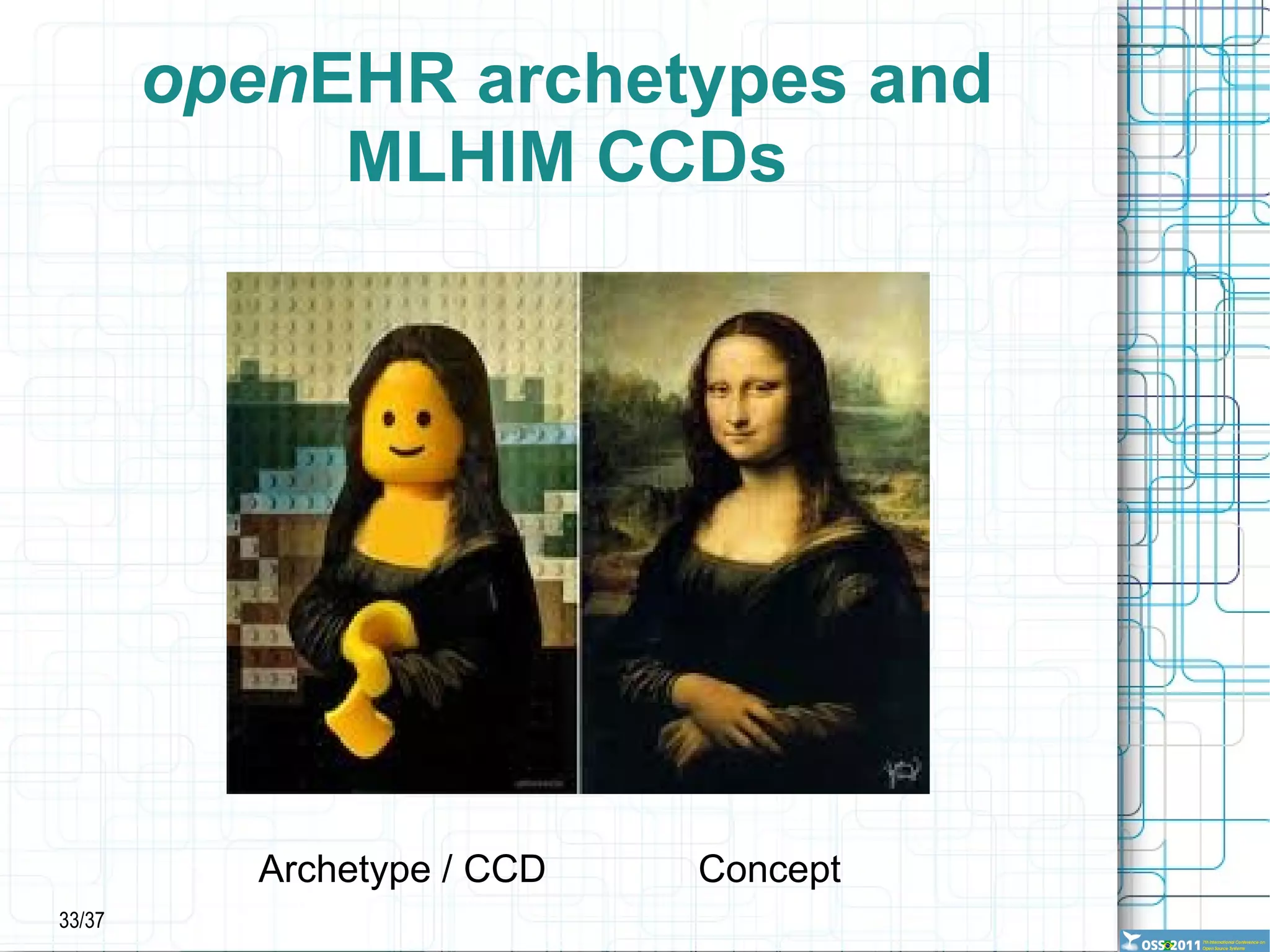







































The document discusses the challenges of healthcare informatics and proposes multilevel modeling (MLM) and open source software as solutions. It argues that MLM separates reference and knowledge models, allowing knowledge to adapt over time without replacing the whole system. Open specifications and tools support sharing knowledge artifacts and ensuring interoperability. MLM and open source align with principles of beneficence, non-maleficence, and efficiency in healthcare informatics. The approach has potential to address issues like information chaos, system failures, and costs that traditional approaches have faced.










































![Presentation Python Brasil [6] 2010](https://cdn.slidesharecdn.com/ss_thumbnails/pythonbr6-130304082039-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)




































