This document provides information about oxygen therapy, including:
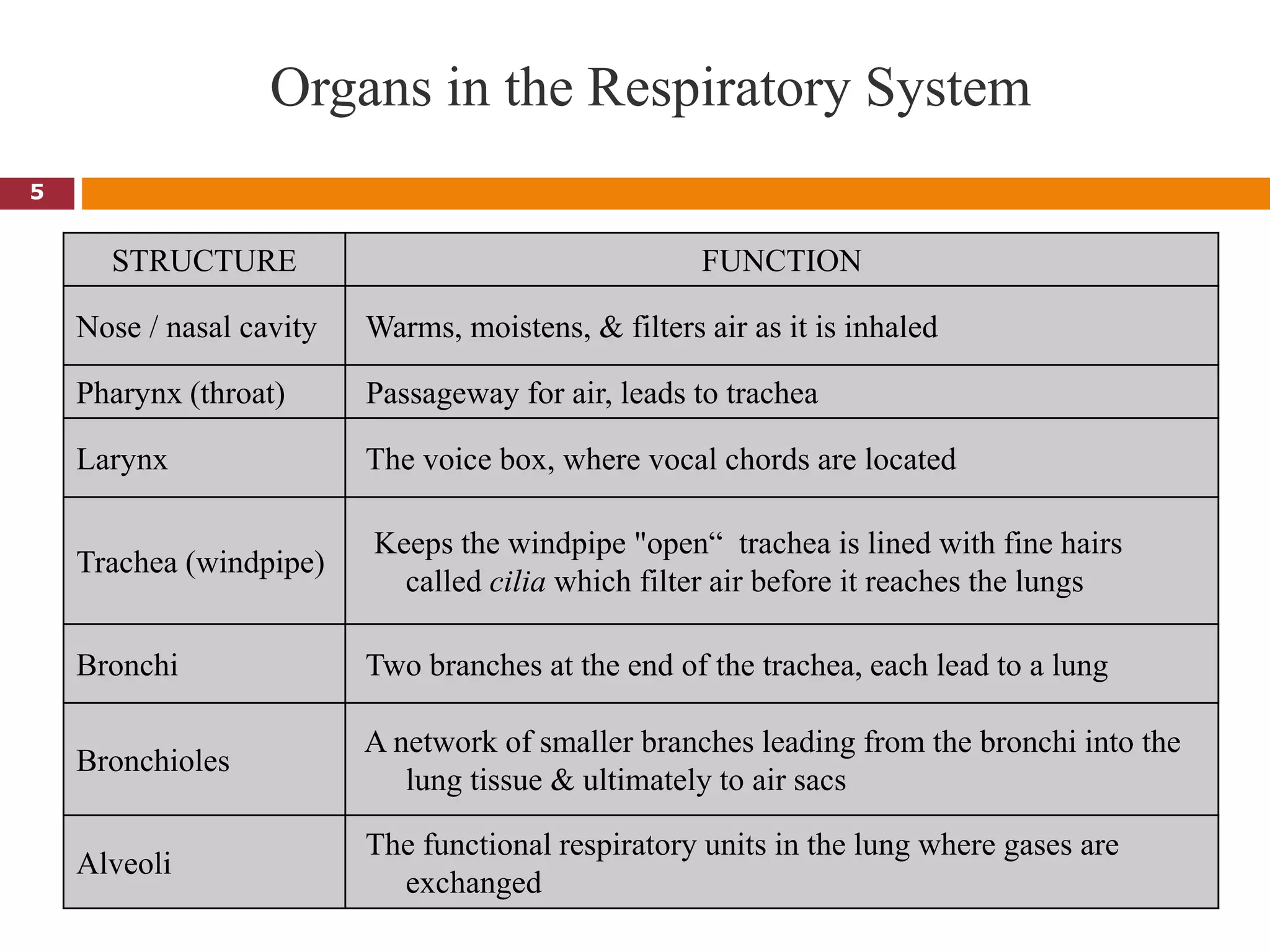
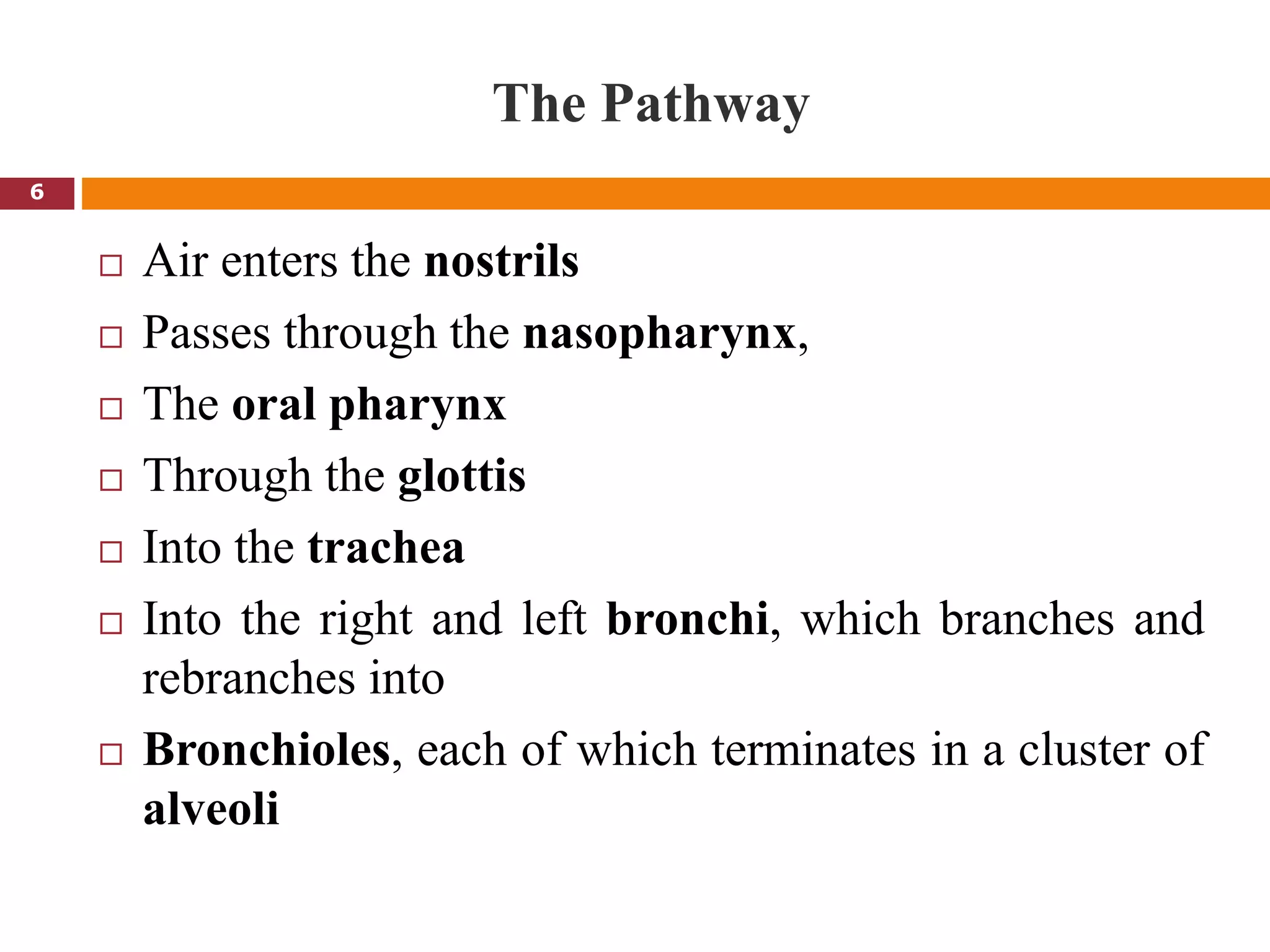
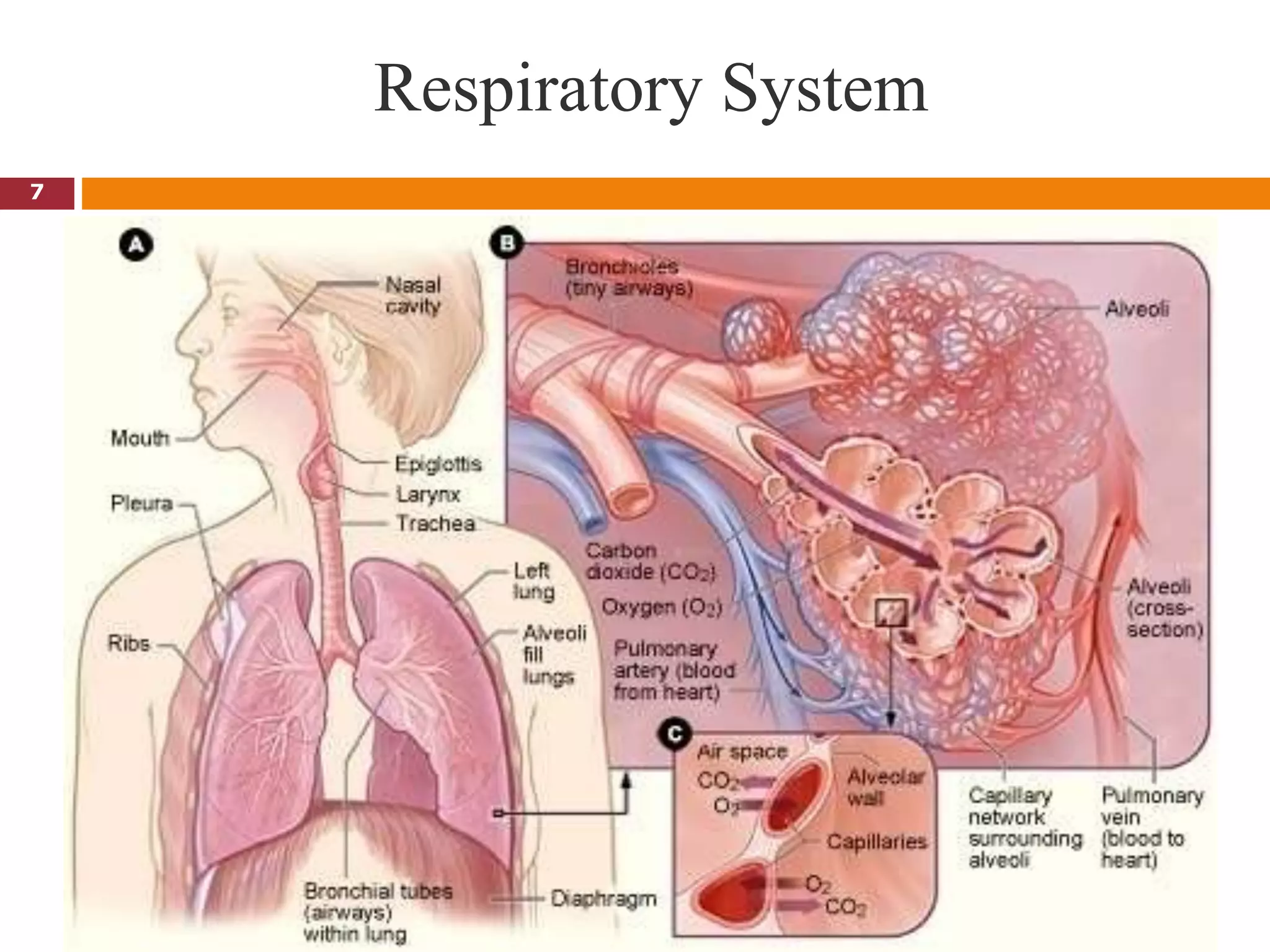
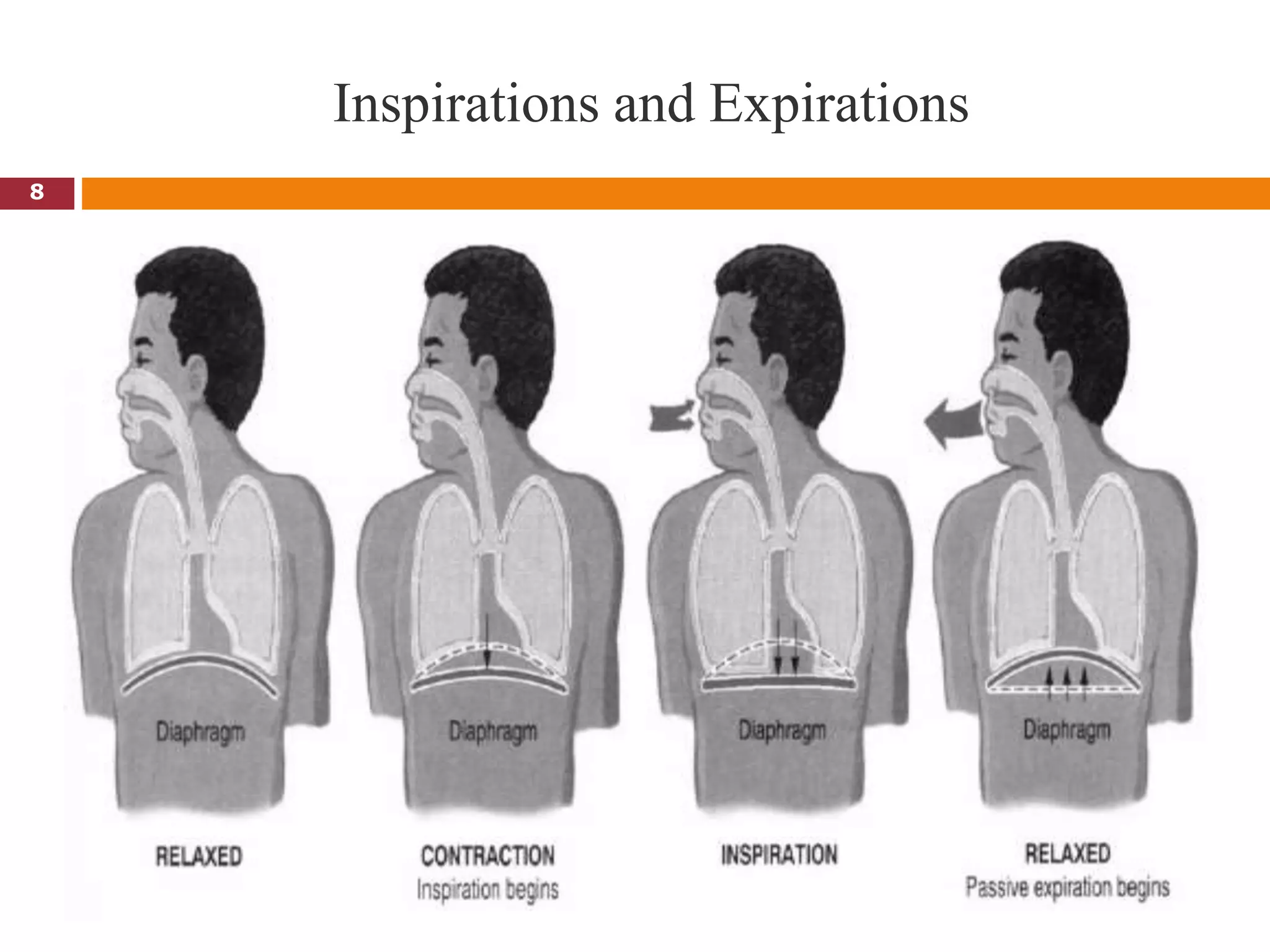
1. It discusses the anatomy and physiology of respiration and defines oxygen therapy as the administration of oxygen at a higher concentration than in the atmosphere.
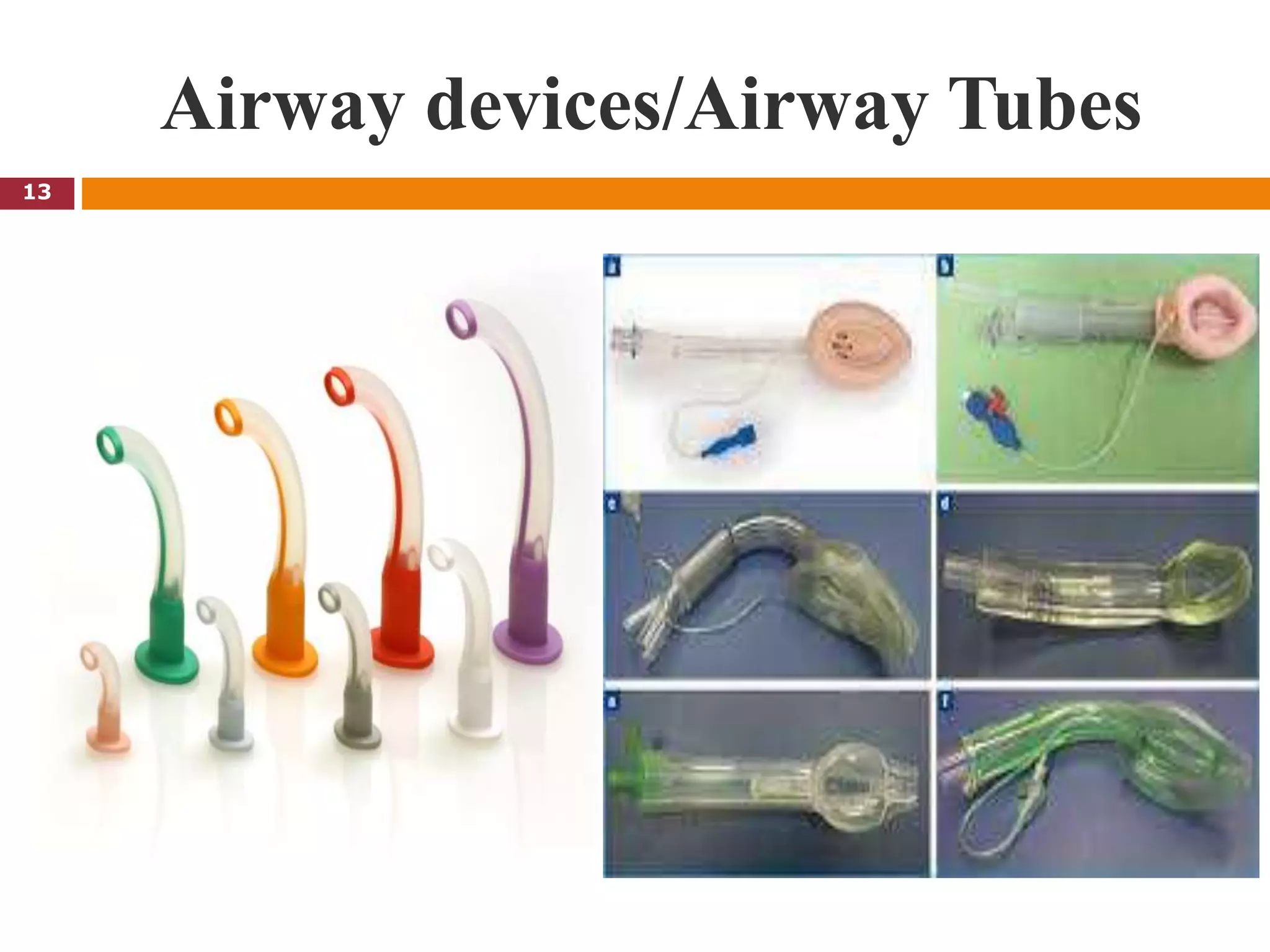
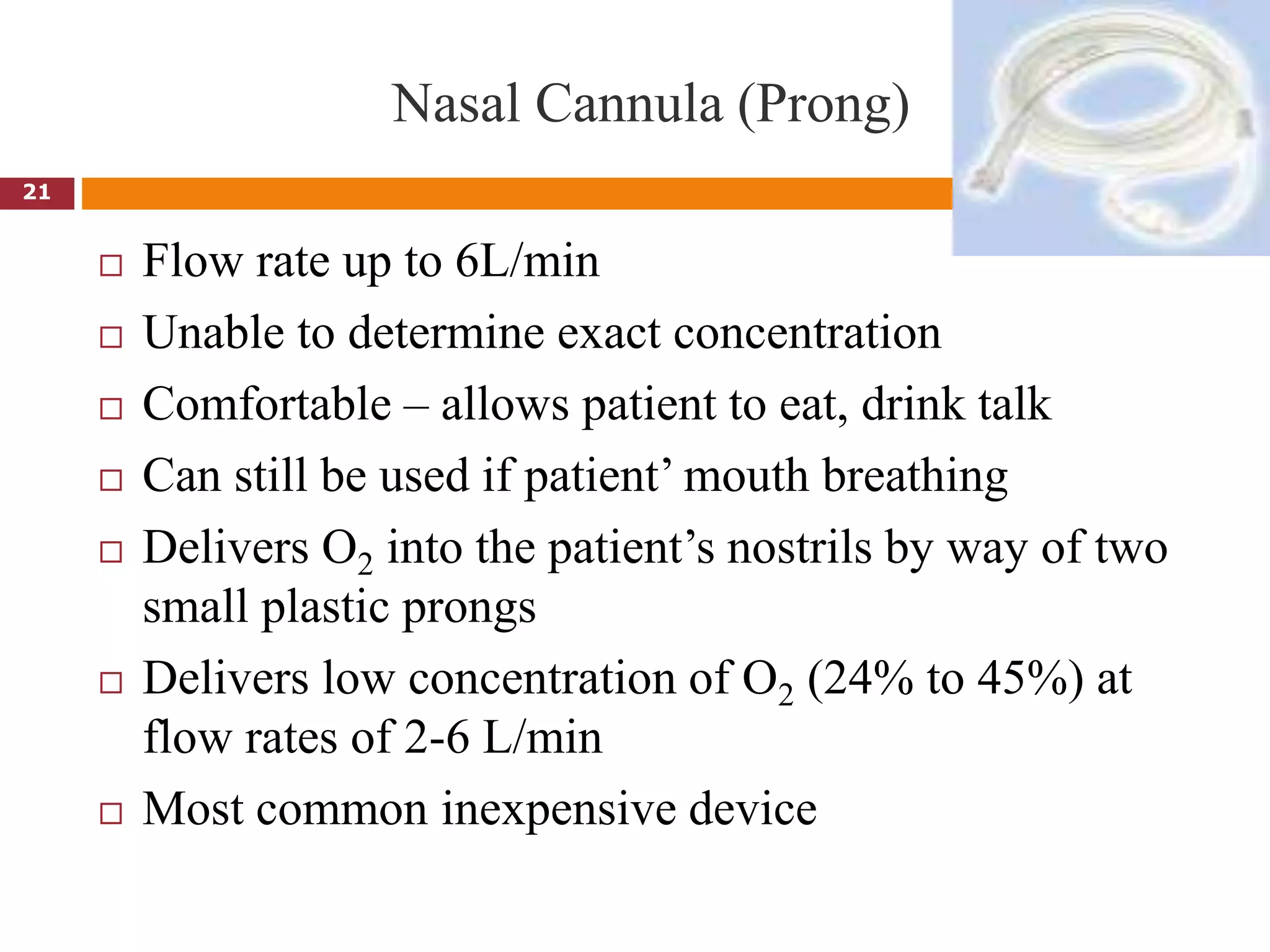
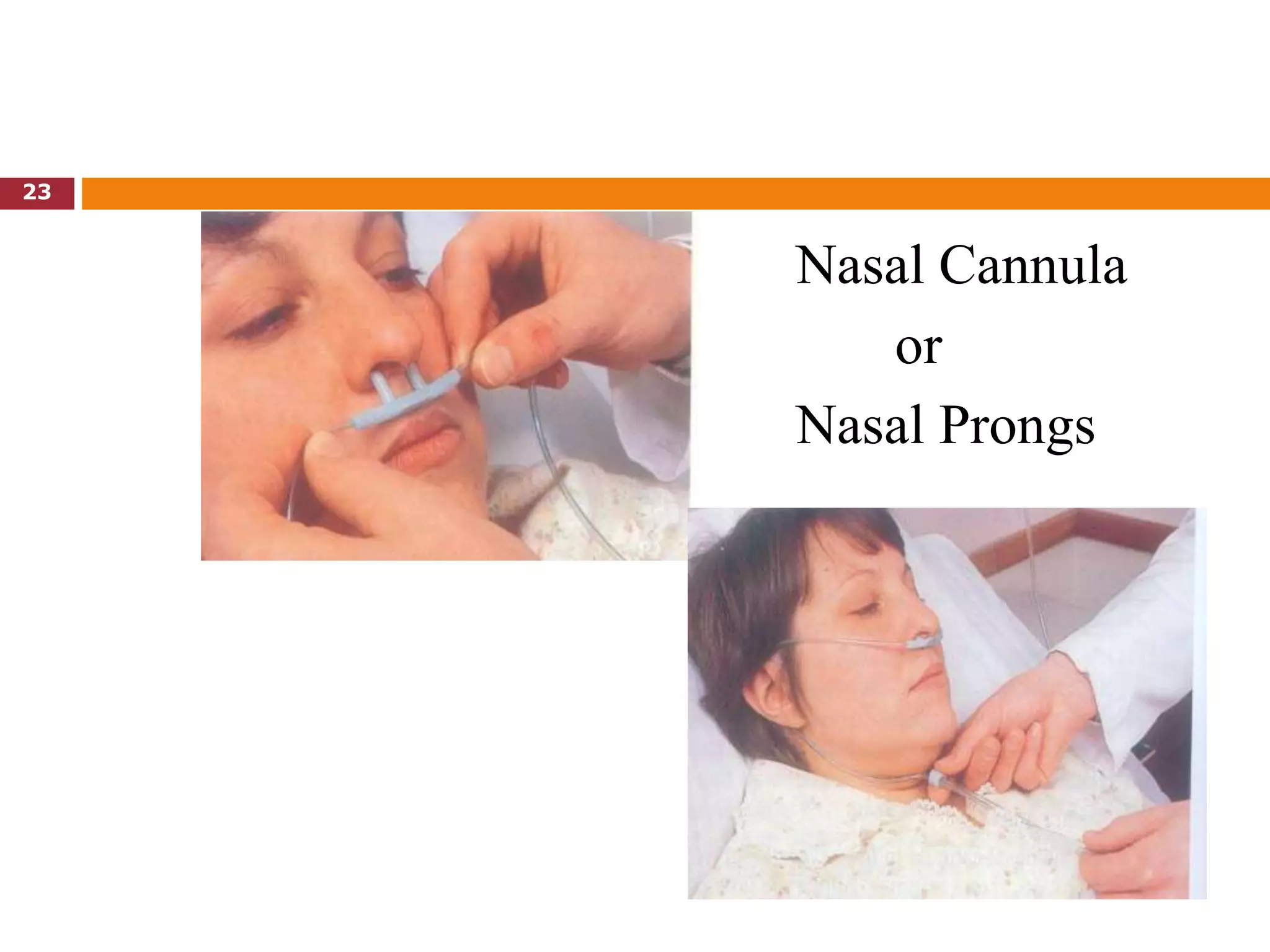
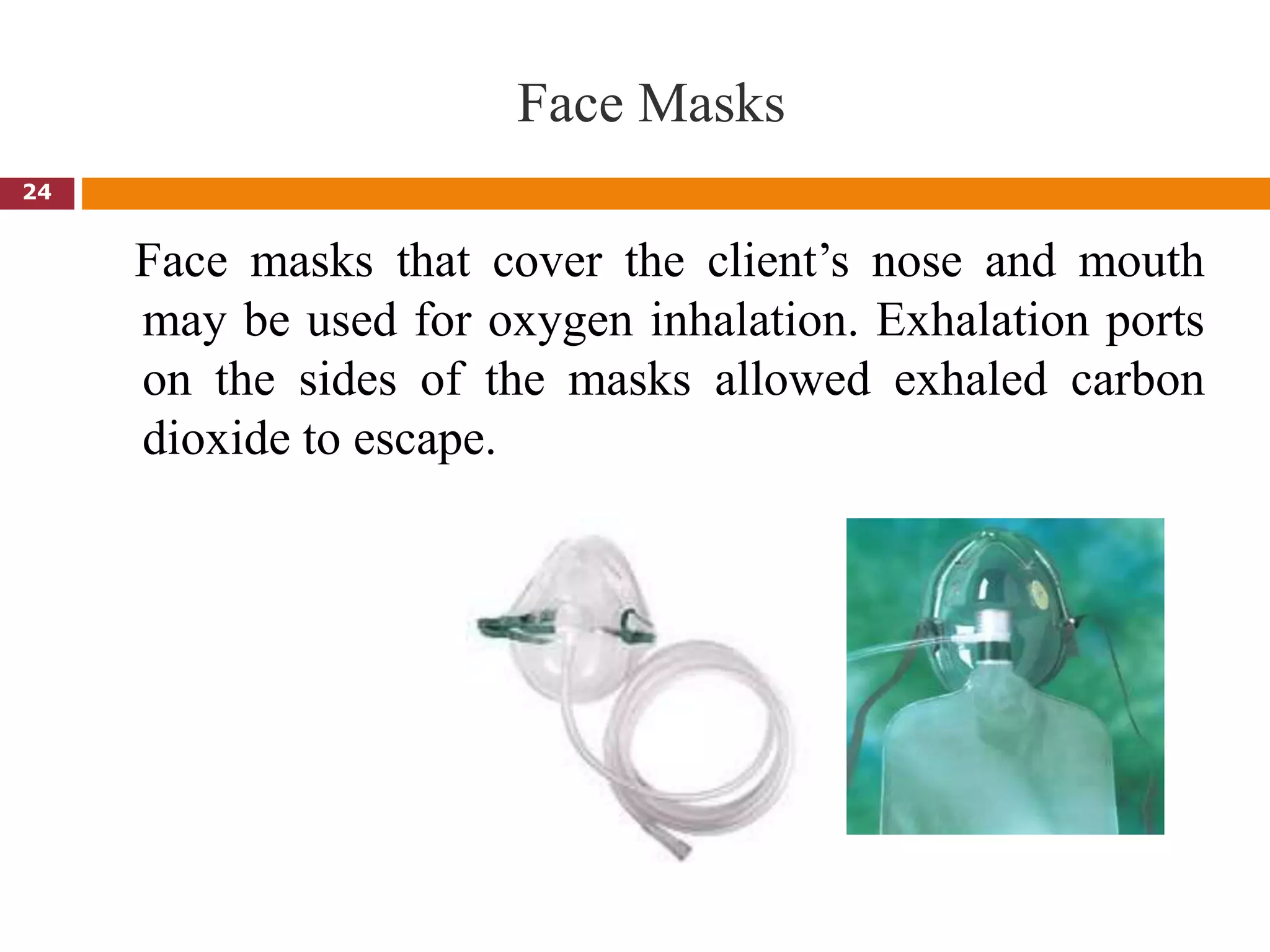
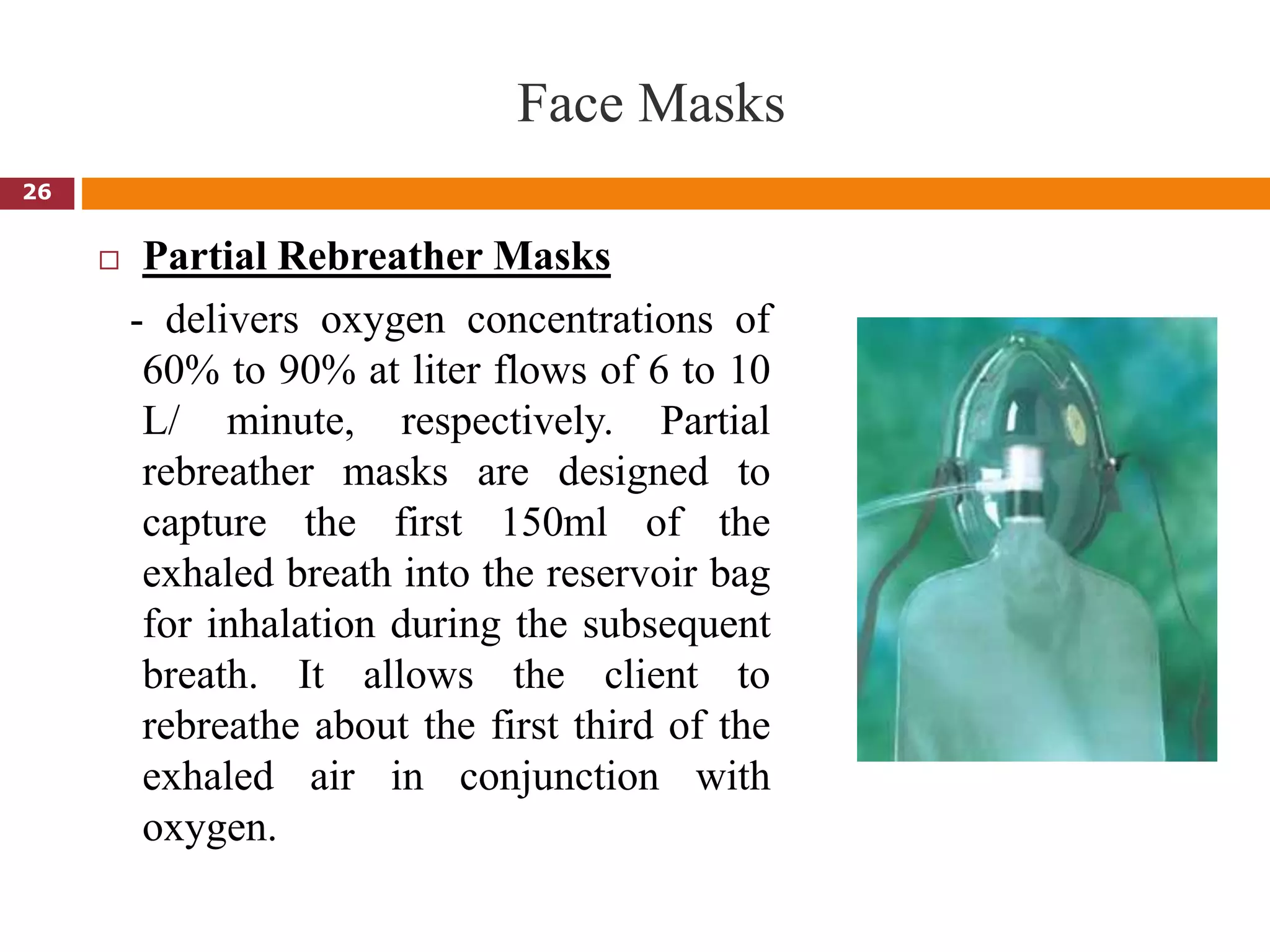
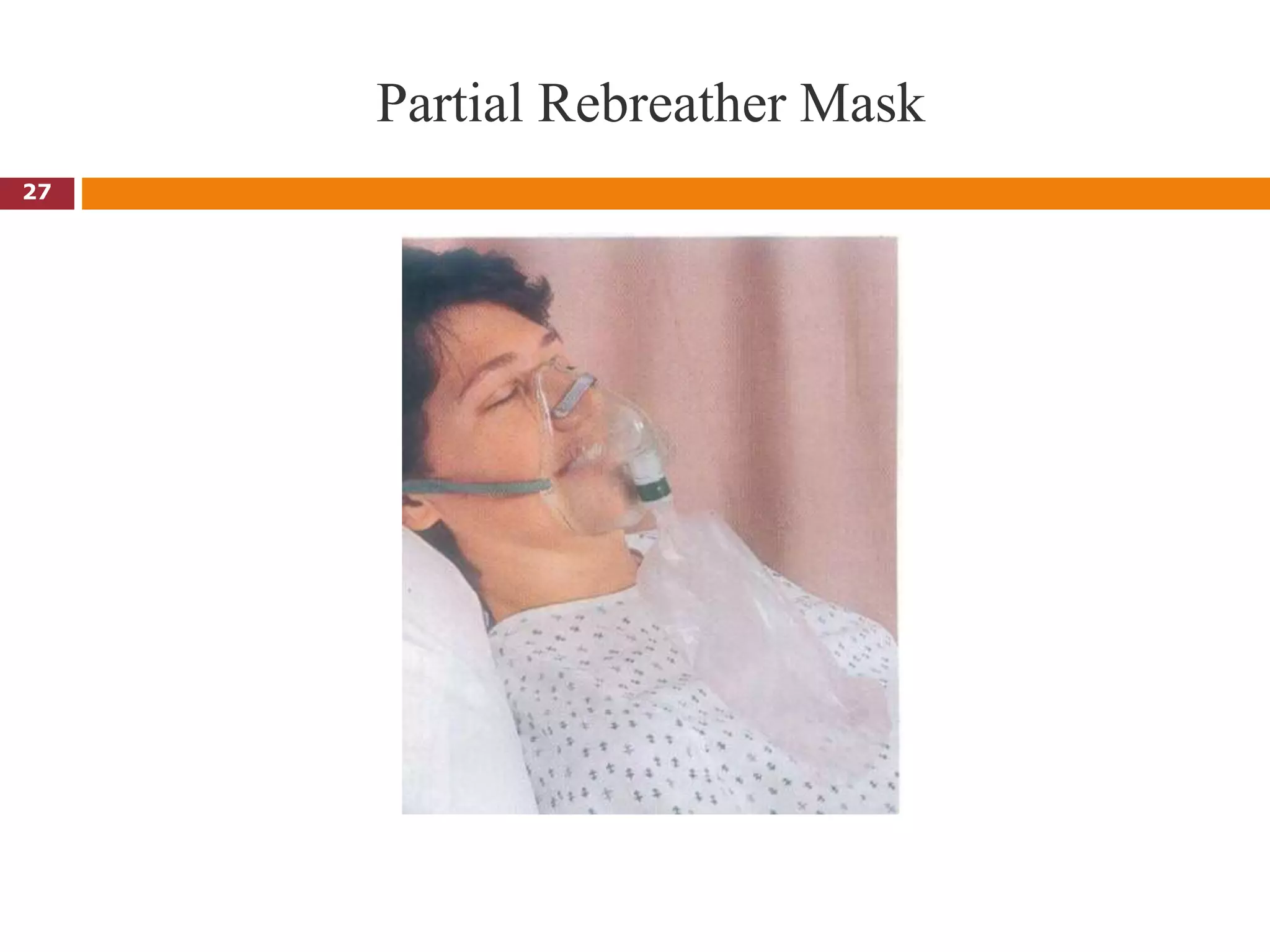
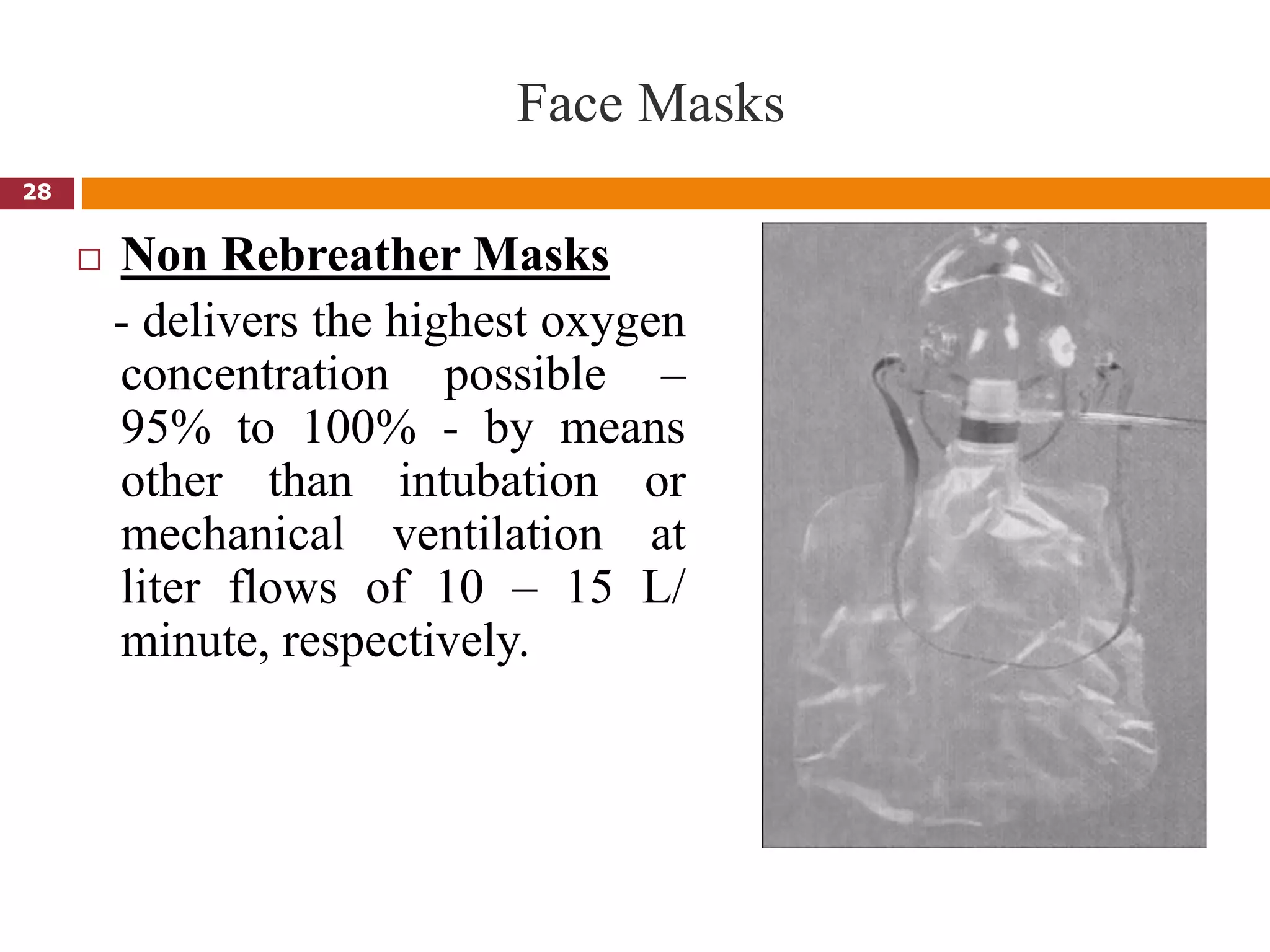
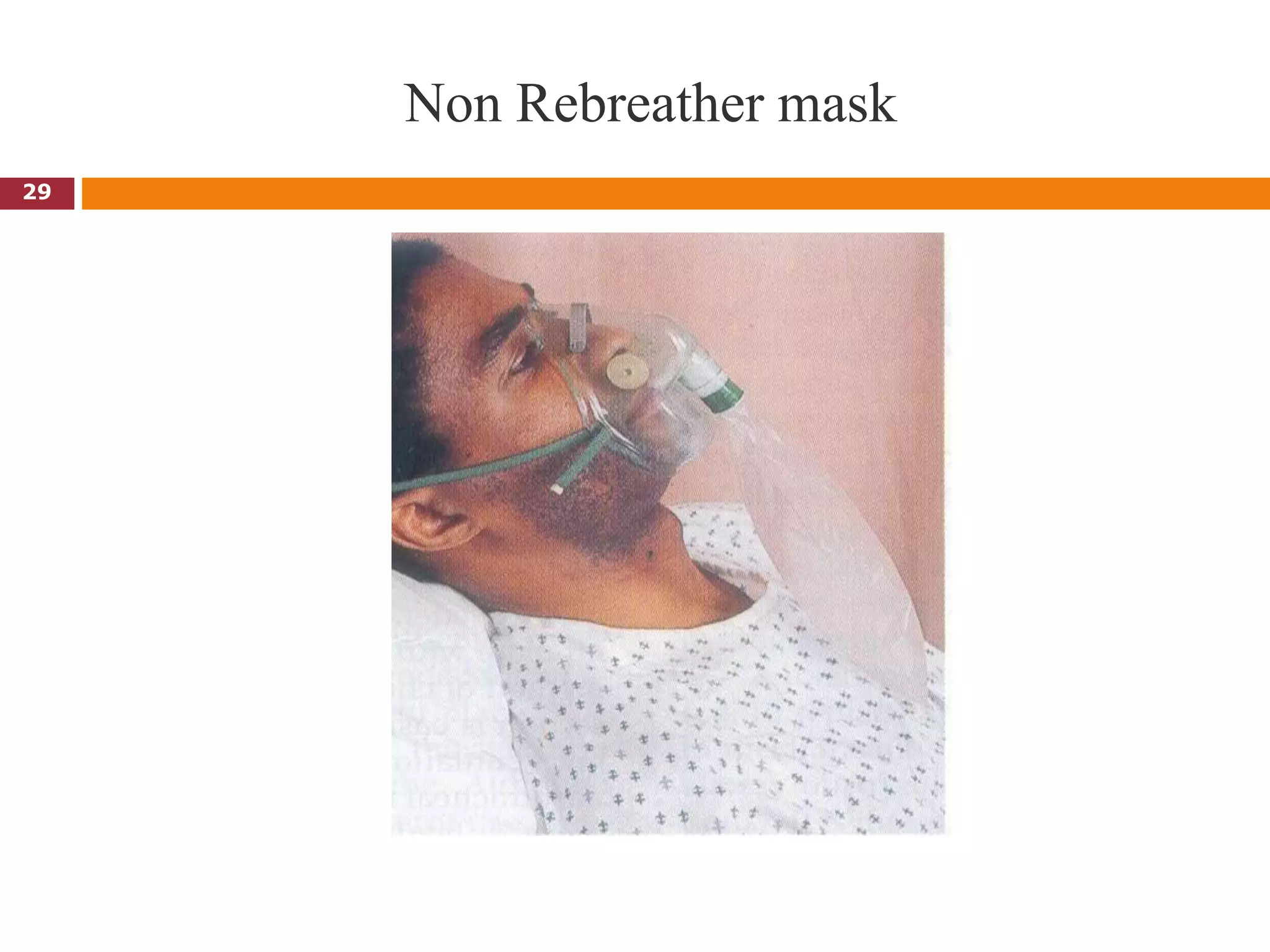
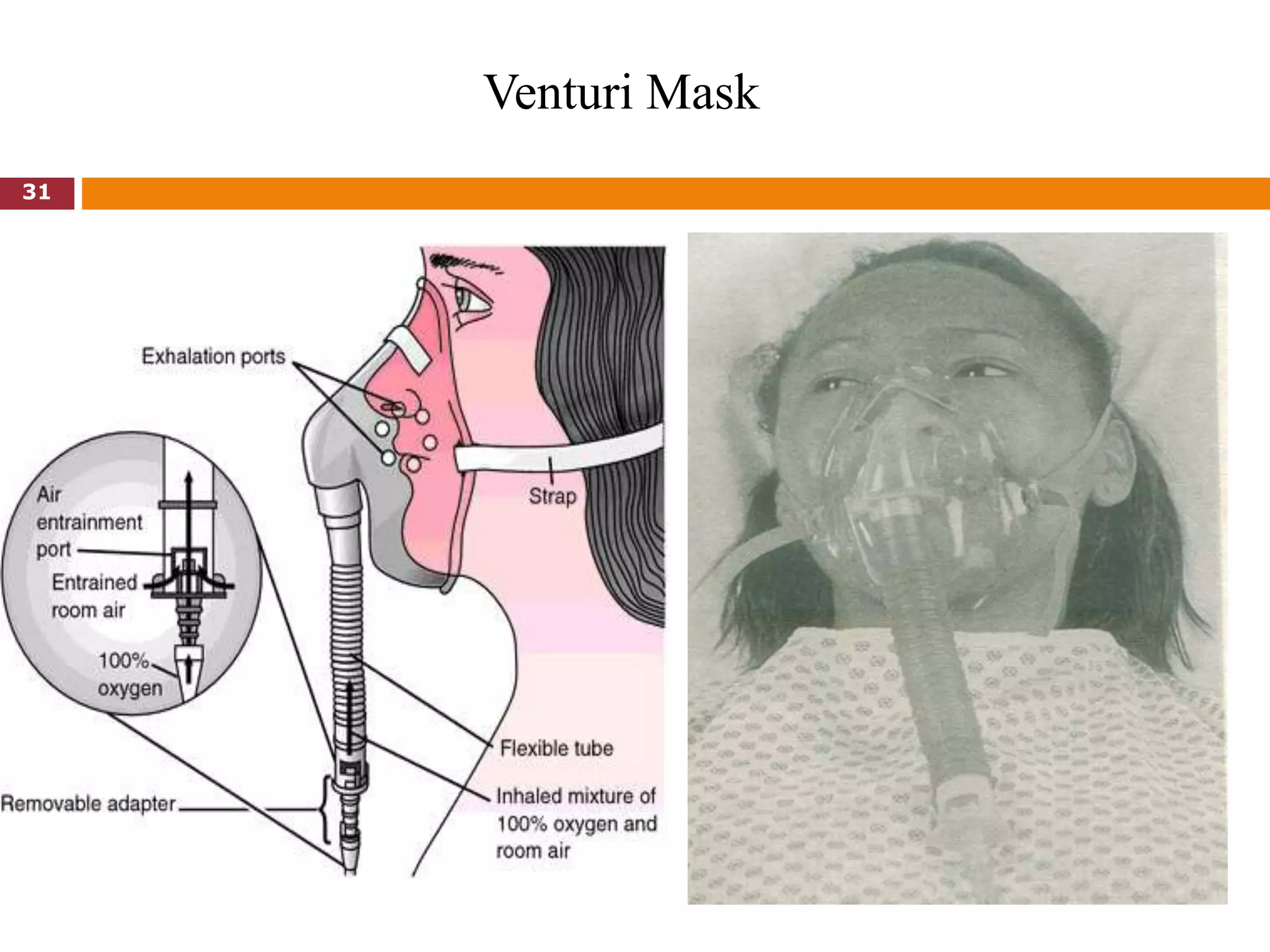
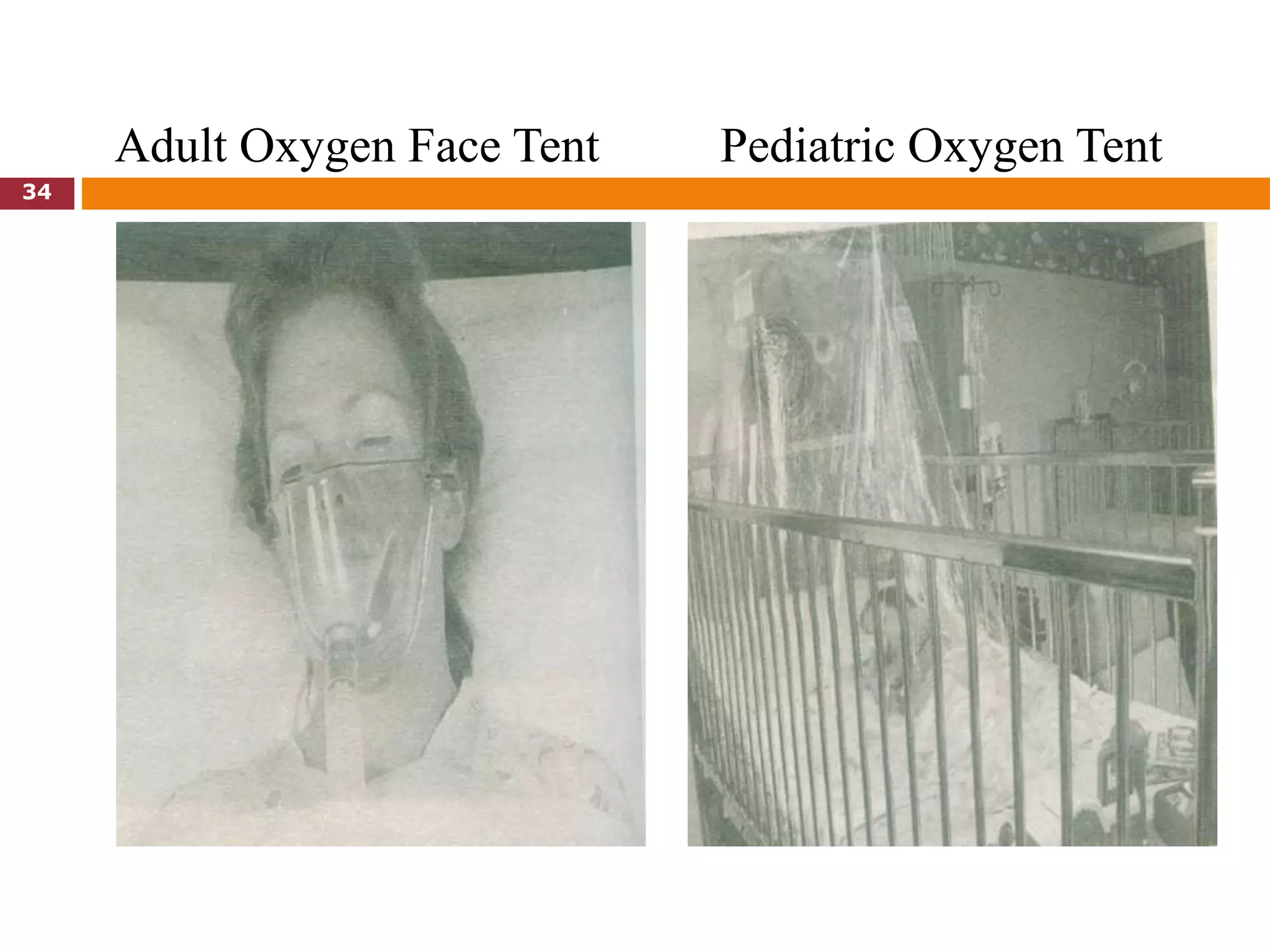
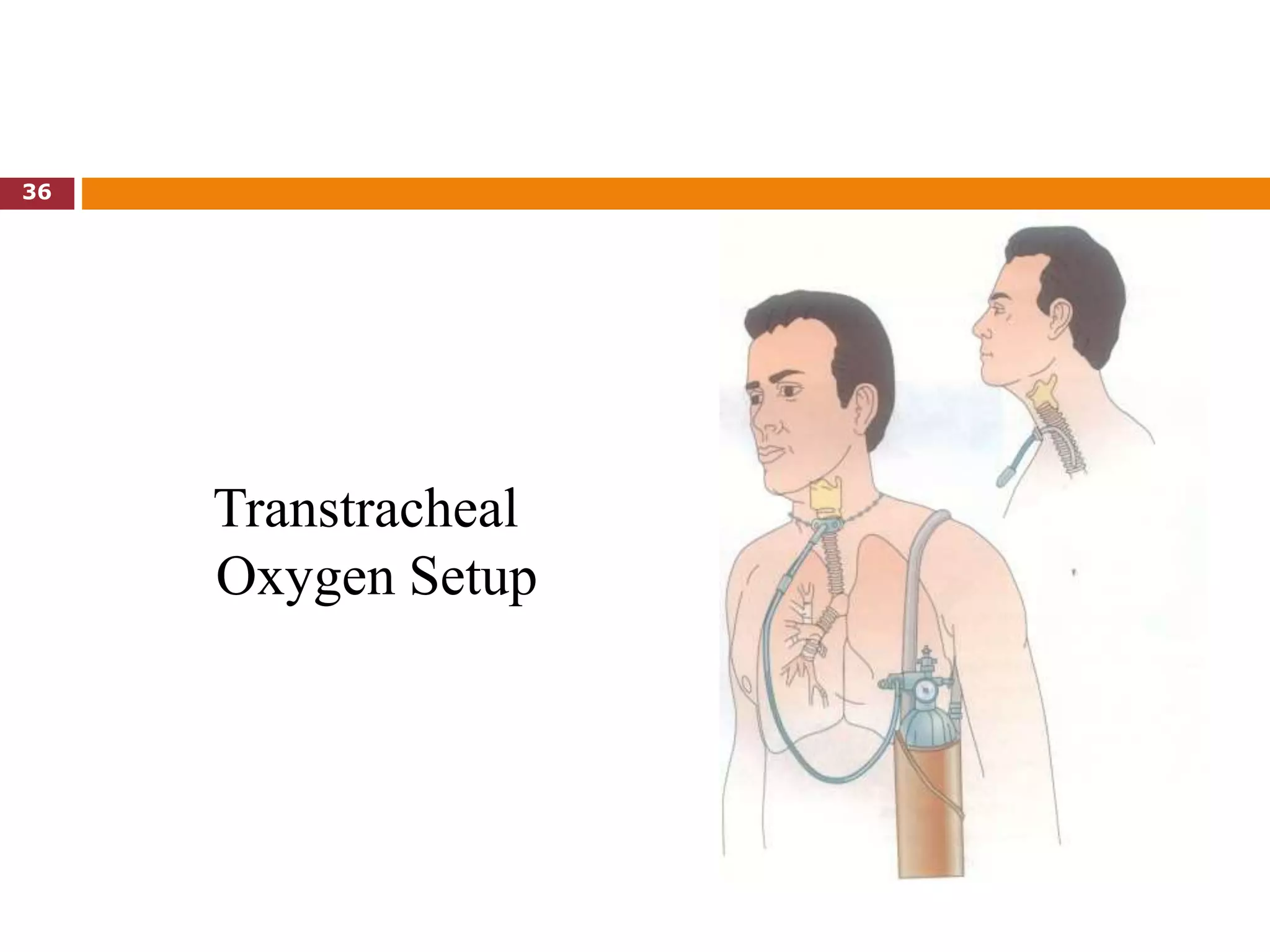
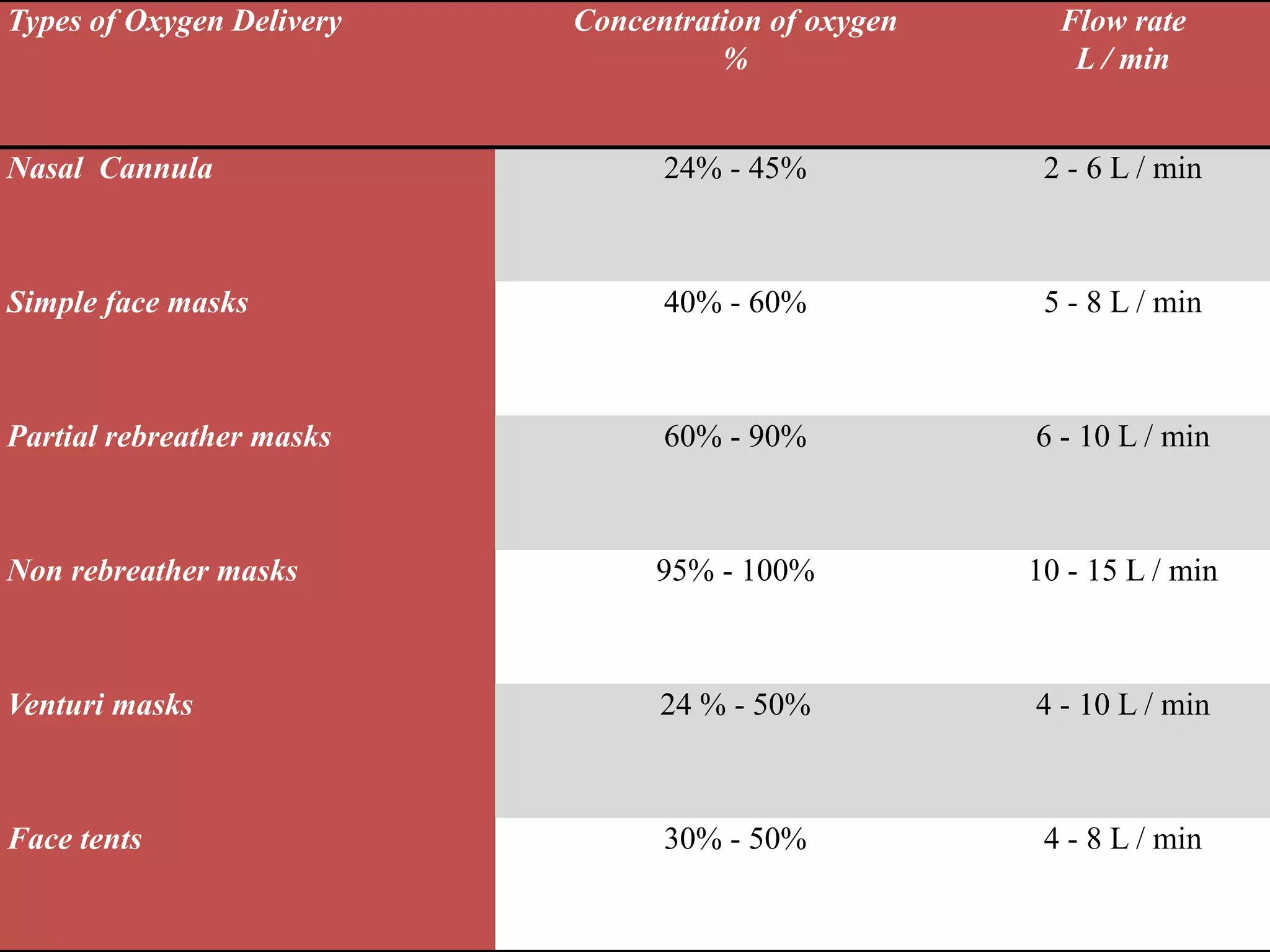
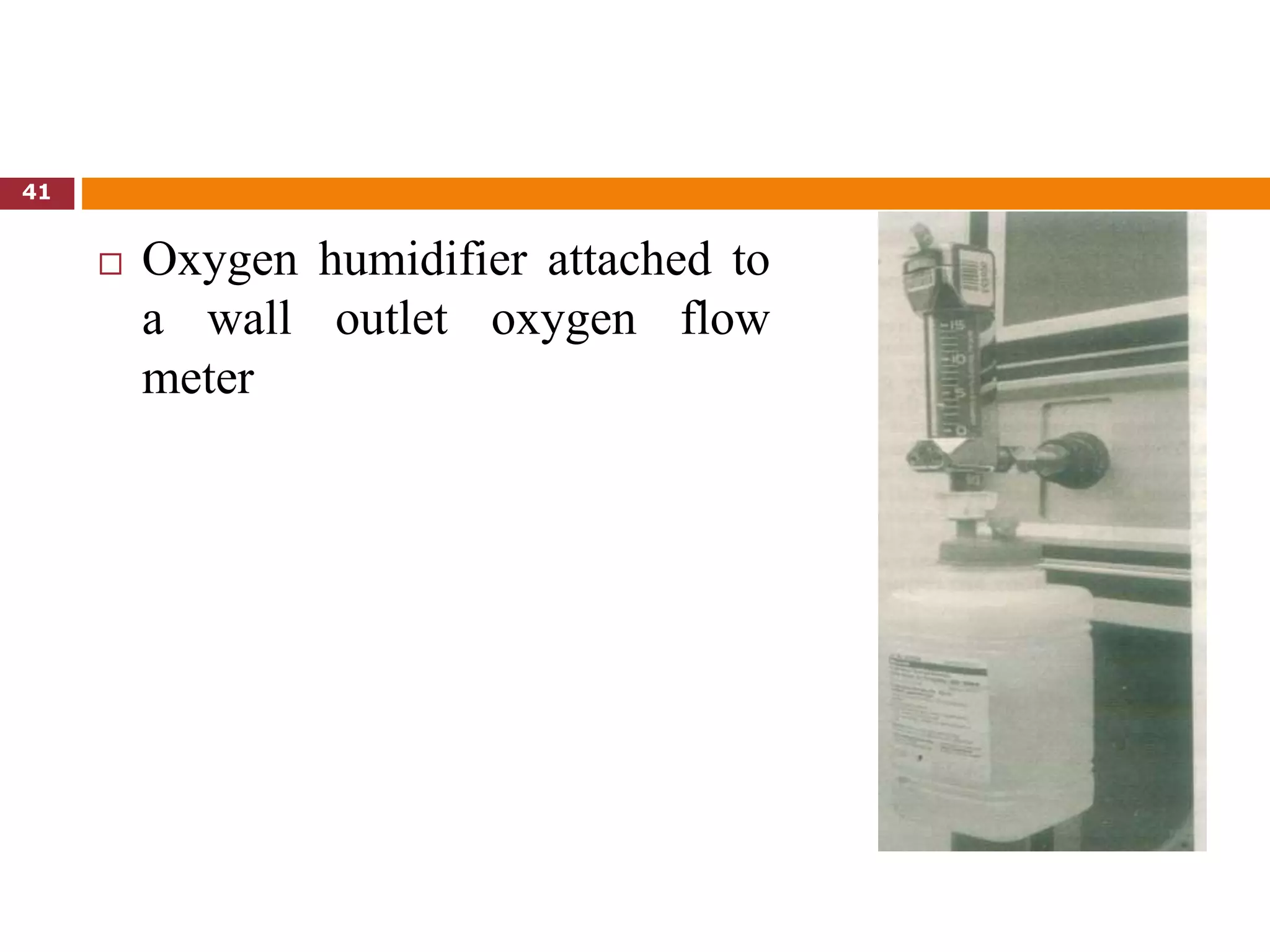
2. The types of oxygen delivery discussed are nasal cannula, face masks, face tents, and transtracheal oxygen delivery. Humidification is also addressed.
3. Nursing responsibilities in administering oxygen therapy are outlined, such as explaining the therapy to patients and demonstrating safe oxygen use. Monitoring patients' response to therapy and pulse oximetry readings are also covered.
























































































































![SHS_Core_CAE_Q3_LE1 FOR THIRD [FINAL].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/shscorecaeq3le1final-251116055110-e3081055-thumbnail.jpg?width=640&height=640&fit=bounds)
