Downloaded 171 times















This document summarizes a seminar presentation on methods for determining bioavailability. It defines bioavailability as the rate and extent to which the active substance of a drug is absorbed and available at the site of action. It then describes the main objectives of bioavailability studies which include aiding new drug and formulation development. The key methods discussed for assessing bioavailability include measuring plasma drug concentration, urinary drug excretion, acute pharmacodynamic effects, clinical observations, and in vitro drug dissolution studies. Specific parameters are defined for each method such as Cmax, AUC, tmax, Du, and Emax. Finally, the document summarizes two literature articles that developed formulations to enhance the oral bioavailability of curcumin and edarav
Introduction to the seminar on Biopharmaceutics focusing on bioavailability methods by Anindya Jana.
Definition of bioavailability; objectives include drug development, formulation comparison, and absorption efficiency.
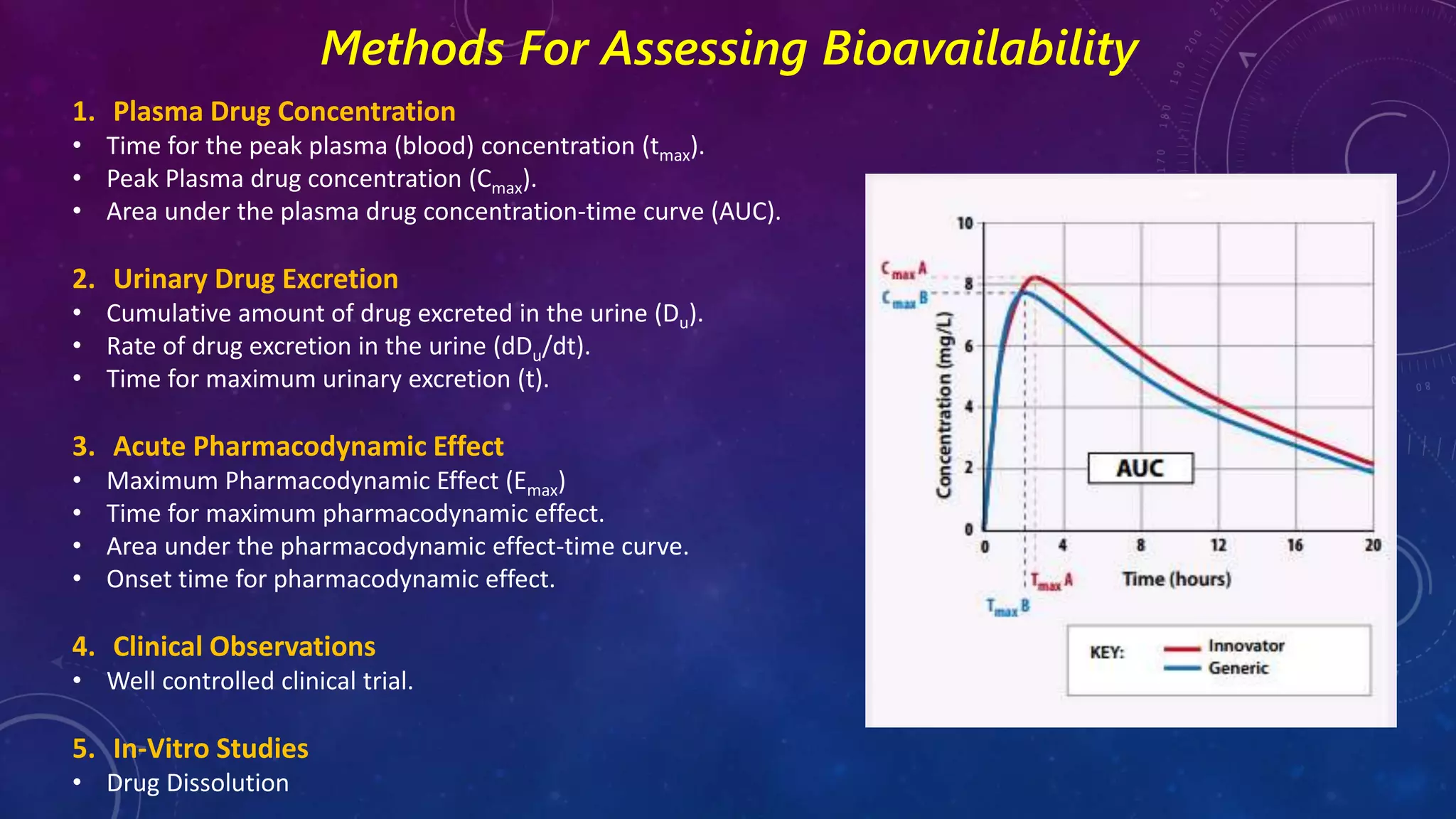
Overview of bioavailability assessment methods: plasma concentration, urinary excretion, pharmacodynamic effect, clinical observations, and in-vitro studies.
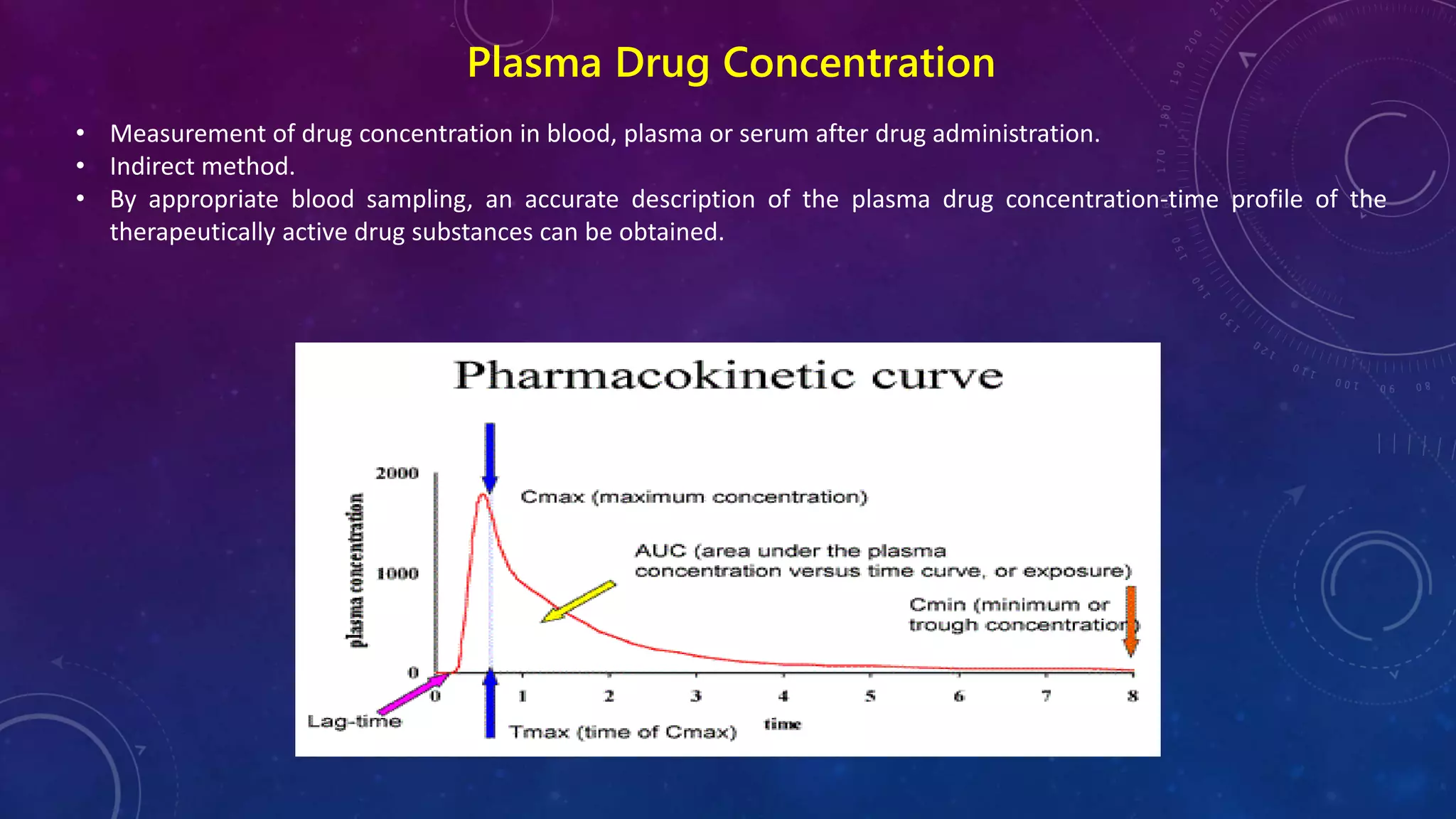
Details on measuring plasma drug concentration post-administration, emphasizing its indirect method.
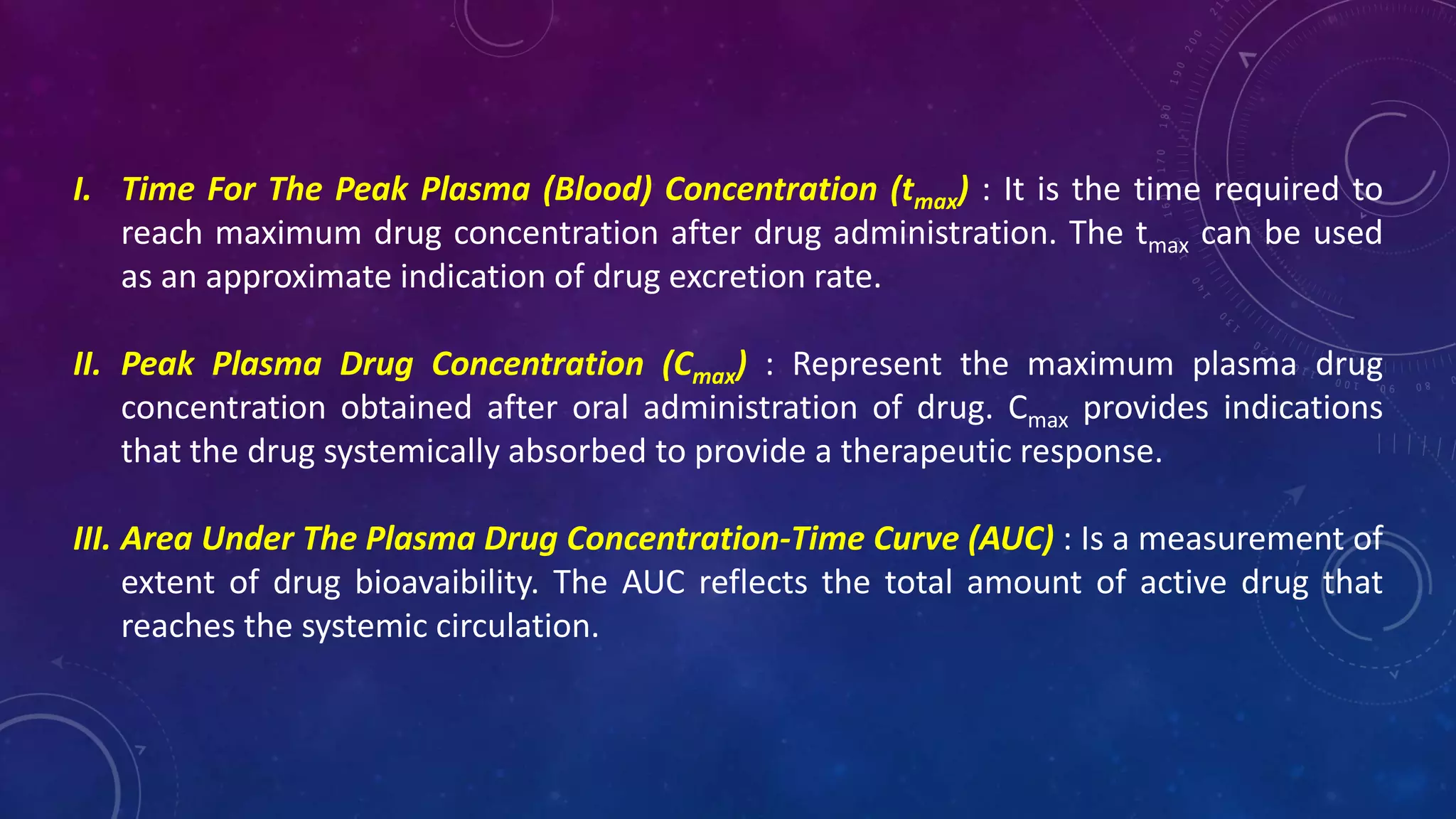
Insights into tmax, Cmax, and AUC as crucial metrics for assessing drug bioavailability.
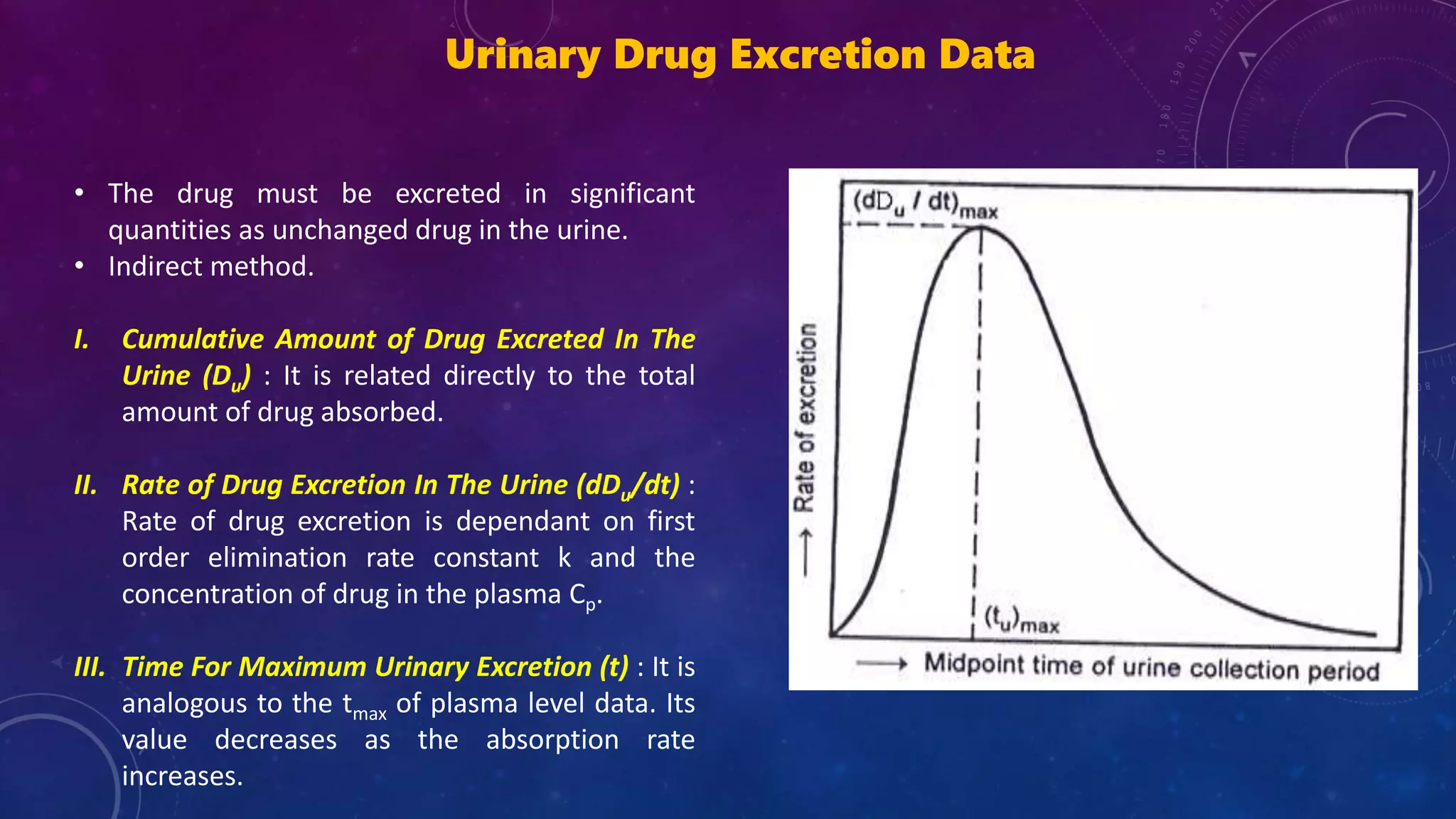
Focus on urinary excretion methods for bioavailability assessment and related metrics like Du and dDu/dt.
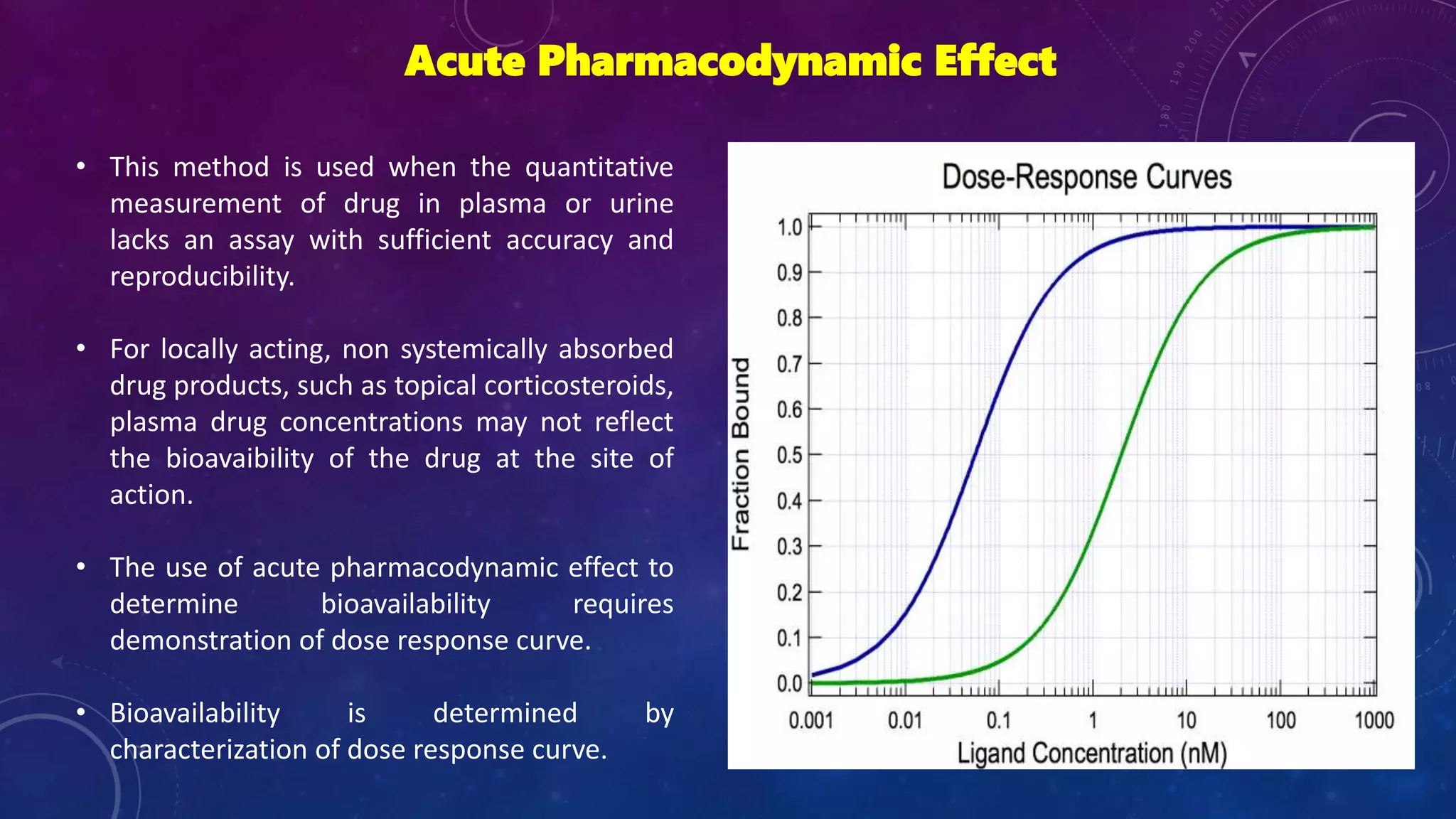
Method used when plasma measurement isn't viable; emphasizes establishing dose-response curves for bioavailability.
Clinical observations in trials to determine safety and effectiveness are discussed; the least accurate method.
Importance of in-vitro drug dissolution studies to correlate with in-vivo bioavailability.
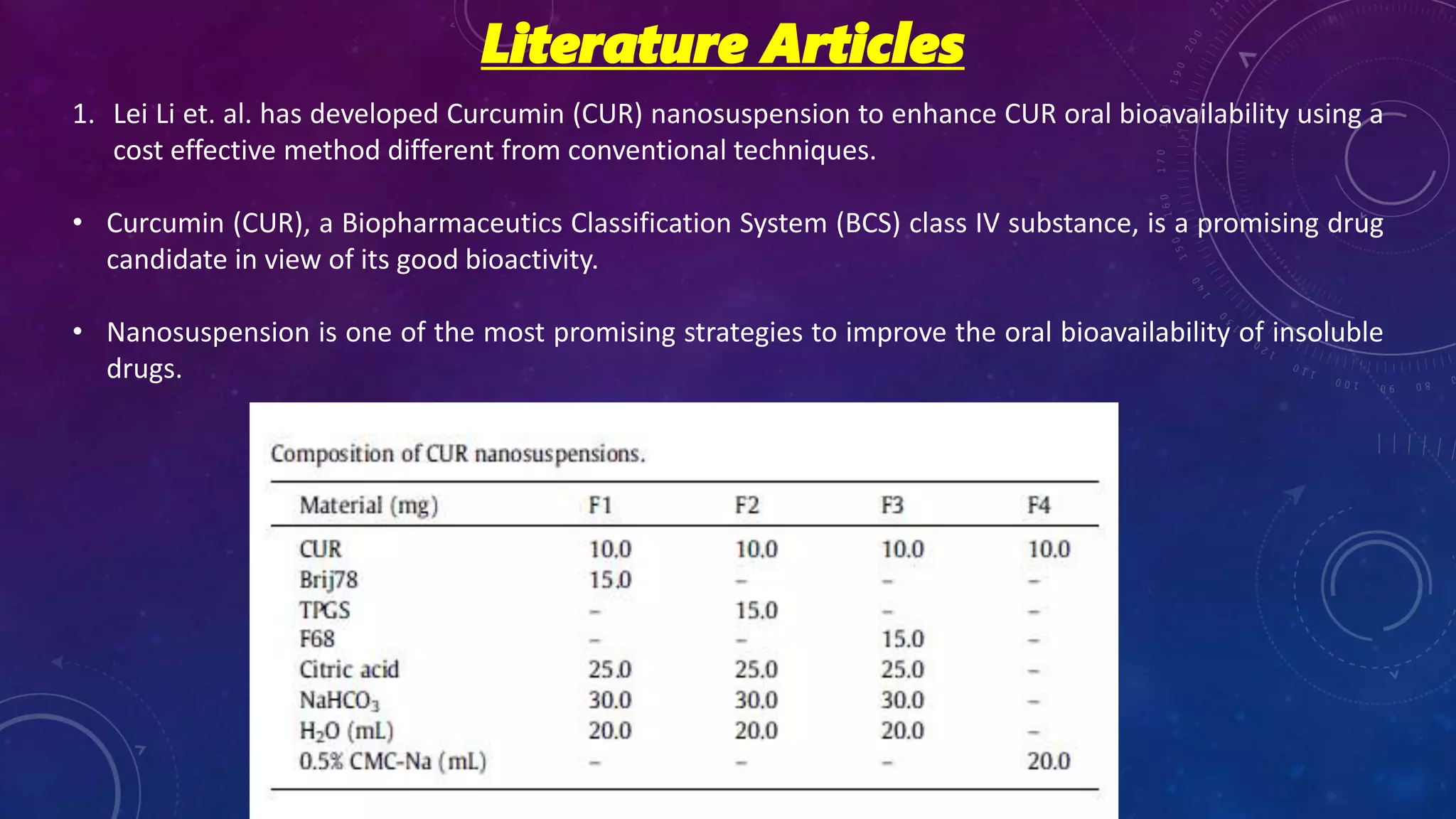
Study development on curcumin nanosuspension to enhance oral bioavailability, focusing on a cost-effective method.
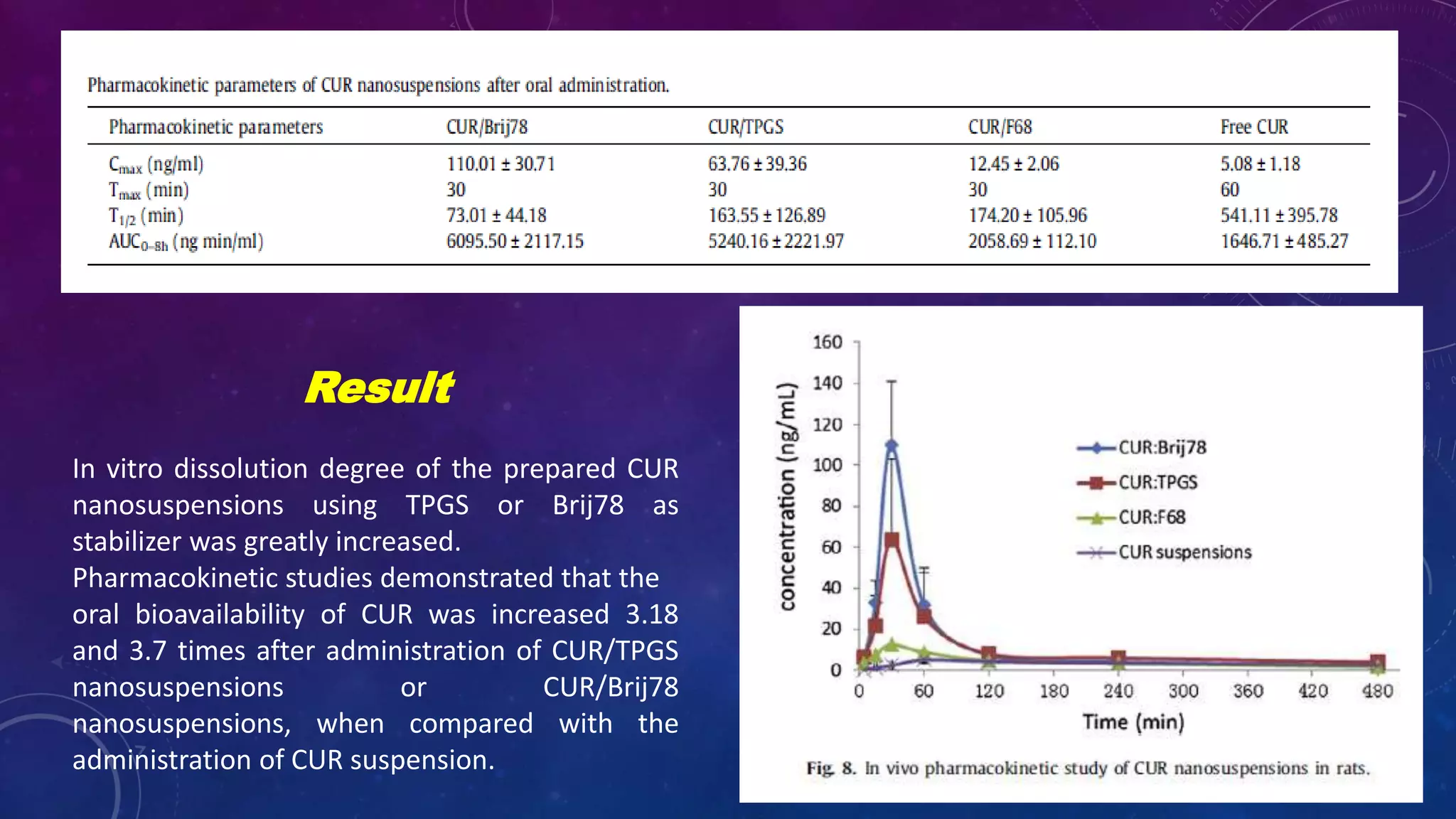
In vitro results show significant increase in curcumin bioavailability with nanosuspensions by factors of 3.18 and 3.7.
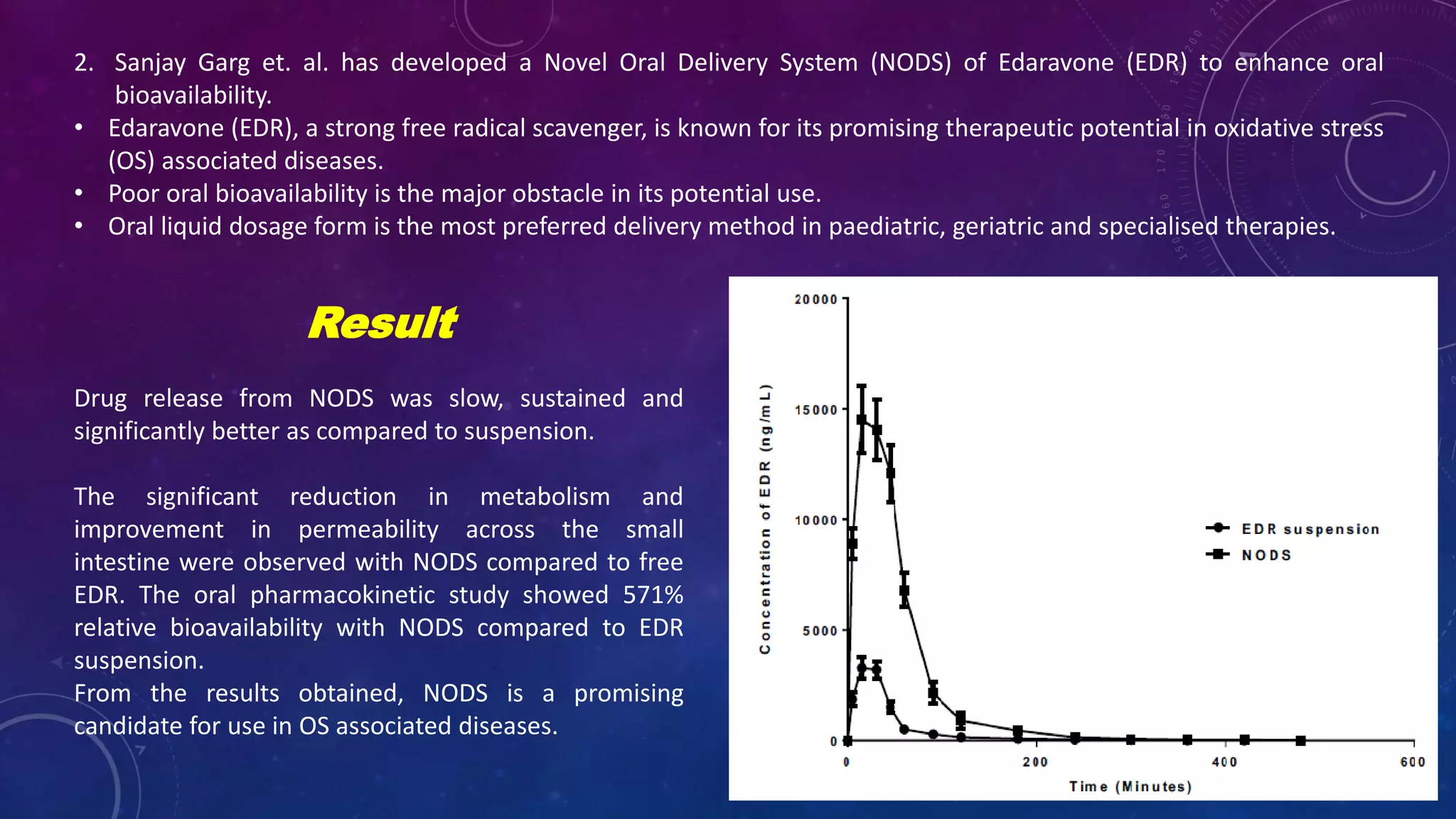
Research on a novel oral delivery system for edaravone to enhance oral bioavailability, with 571% improvement highlighted.
List of references relevant to bioavailability methods and studies, further informing the research.
A closing slide thanking the audience.











































































