Latent tuberculosis infection(LTBI): A state of persistent immune response to
stimulation by M. tuberculosis antigens with no evidence of clinically manifest active TB
TB preventive treatment (TPT): Treatment offered to individuals who are considered at
risk of TB disease in order to reduce that risk
TB disease - this occurs when a person exposed to TB bacteria develops signs and
symptoms of TB
Household contact (HHC): A person who shared the same enclosed living space as the
index case for one or more nights or for frequent or extended daytime periods during
the 3 months before the start of current treatment
Definition of key terms
3.
One-quarter of theworld population is estimated to have LTBI
5–15% of those infected will develop active TB disease over the course of their lives,
usually within the first 5 years after initial infection (WHO LTBI Guideline 2019)
People with LTBI form reservoirs for a significant proportion of emerging active TB
• People with LTBI are “seedbeds” of tuberculosis in the community
The positivity of LTBI among health care workers in Kiambu County was 78%( preliminary
report)
The proportion of the Kenyan population that is infected with Mycobacterium
tuberculosis is unknown
Burden and implications of LTBI
4.
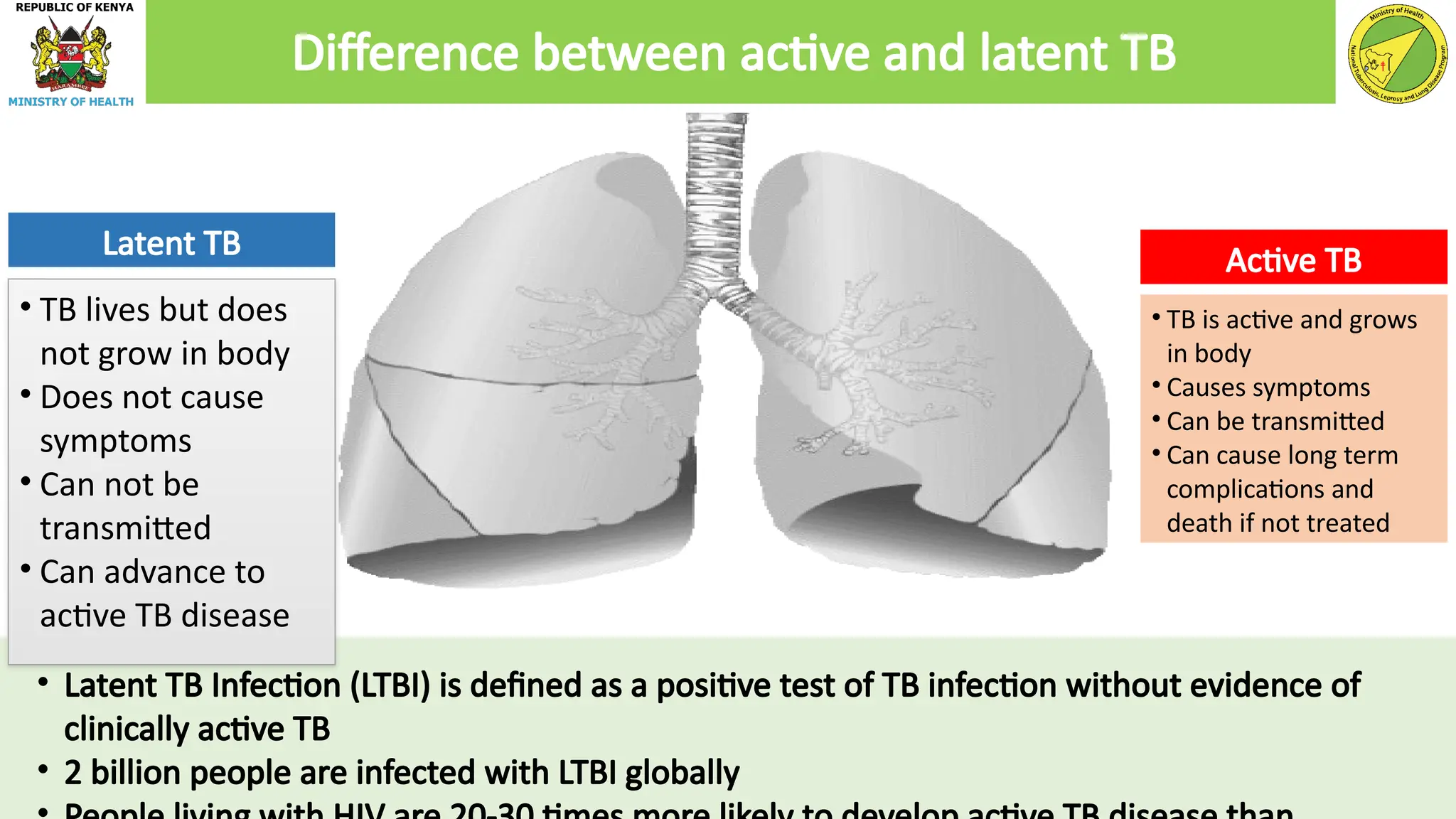
• TB livesbut does
not grow in body
• Does not cause
symptoms
• Can not be
transmitted
• Can advance to
active TB disease
• TB is active and grows
in body
• Causes symptoms
• Can be transmitted
• Can cause long term
complications and
death if not treated
Latent TB Active TB
• Latent TB Infection (LTBI) is defined as a positive test of TB infection without evidence of
clinically active TB
• 2 billion people are infected with LTBI globally
Difference between active and latent TB
5.
Since 5–15% ofthose with
Latent TB will progress to
active TB in their lives, it is
therefore important to
offer TB preventive
therapy
Kenya’s targets for
treatment of persons
with LTBI is 900,000
(NSP 2019-2023)
Prevention of active TB
disease by TPT is a: -
Critical component of
the End TB Strategy
- Key strategy in
achieving the global
agenda of ending TB by
2035
The TB/ HIV confection
rate has reduced with the
introduction of TB
preventive therapy and
ART
Why should Latent TB Infection be treated?
6.
To reduce therisk of progression from latent TB to active disease by killing
the dormant mycobacteria
TPT
• Reduces morbidity
• Reduces progression from LTBI to active Tb disease, hence reducing
transmission of TB
Cost saving: treatment of active TB involves four antibiotics, LTBI treatment
uses one or two antibiotics
Mycobacteria bacilli are not actively replicating, there is a reduced
likelihood of developing acquired drug resistance
Rationale for TB preventive therapy
Clinical risk groups
•Patients receiving immunosuppressants
• Patients receiving dialysis
• Patients preparing for an organ or haematological
transplant
• Patients with silicosis
Eligible populations for TPT
Prisoners and
staff working in
prison settings
Health care
workers and
other staff in
healthcare
settings
People living with
HIV (PLHIV):
Children aged ≥ 12
months,
adolescents and
adults
All household
contacts of a
bacteriologically
confirmed PTB
patients
9.
HIV is thestrongest risk factor associated with the development of active TB with up to 40% of patients
progressing to TB disease after exposure
PLHIV also have approximately 21 times higher risk of TB disease compared to the HIV negative persons.
About 2% of PLHIVs get TB annually
Mortality among TB/HIV co-infected patients during TB treatment is three times more than TB
uninfected PLHIV
The early detection and treatment of LTBI in PLHIV reduces the overall risk of TB disease progression by
33%
People Living with HIV
10.
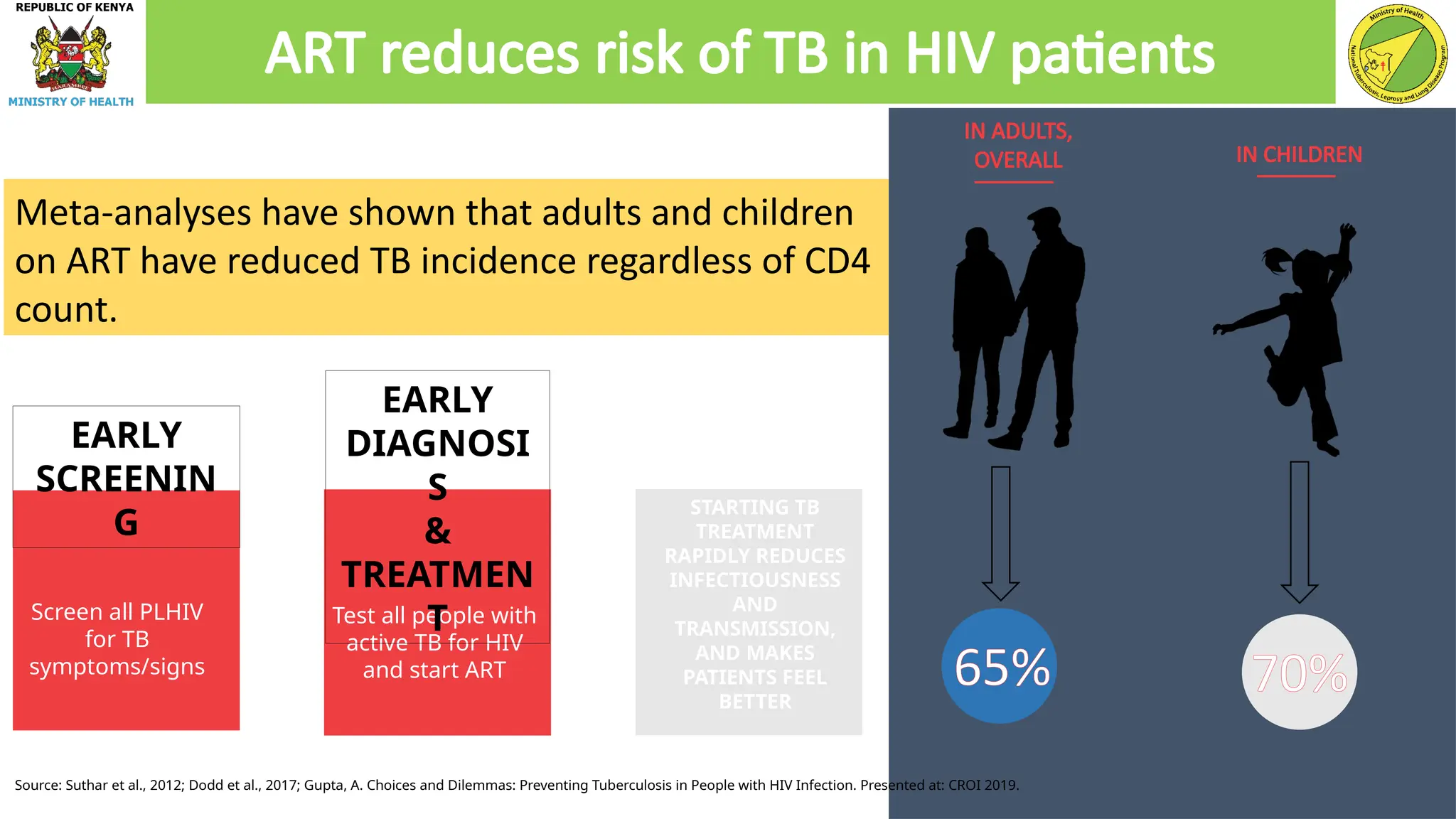
Meta-analyses have shownthat adults and children
on ART have reduced TB incidence regardless of CD4
count.
Test all people with
active TB for HIV
and start ART
Screen all PLHIV
for TB
symptoms/signs
STARTING TB
TREATMENT
RAPIDLY REDUCES
INFECTIOUSNESS
AND
TRANSMISSION,
AND MAKES
PATIENTS FEEL
BETTER
IN ADULTS,
OVERALL IN CHILDREN
70%
ART reduces risk of TB in HIV patients
65%
Source: Suthar et al., 2012; Dodd et al., 2017; Gupta, A. Choices and Dilemmas: Preventing Tuberculosis in People with HIV Infection. Presented at: CROI 2019.
EARLY
SCREENIN
G
EARLY
DIAGNOSI
S
&
TREATMEN
T
11.
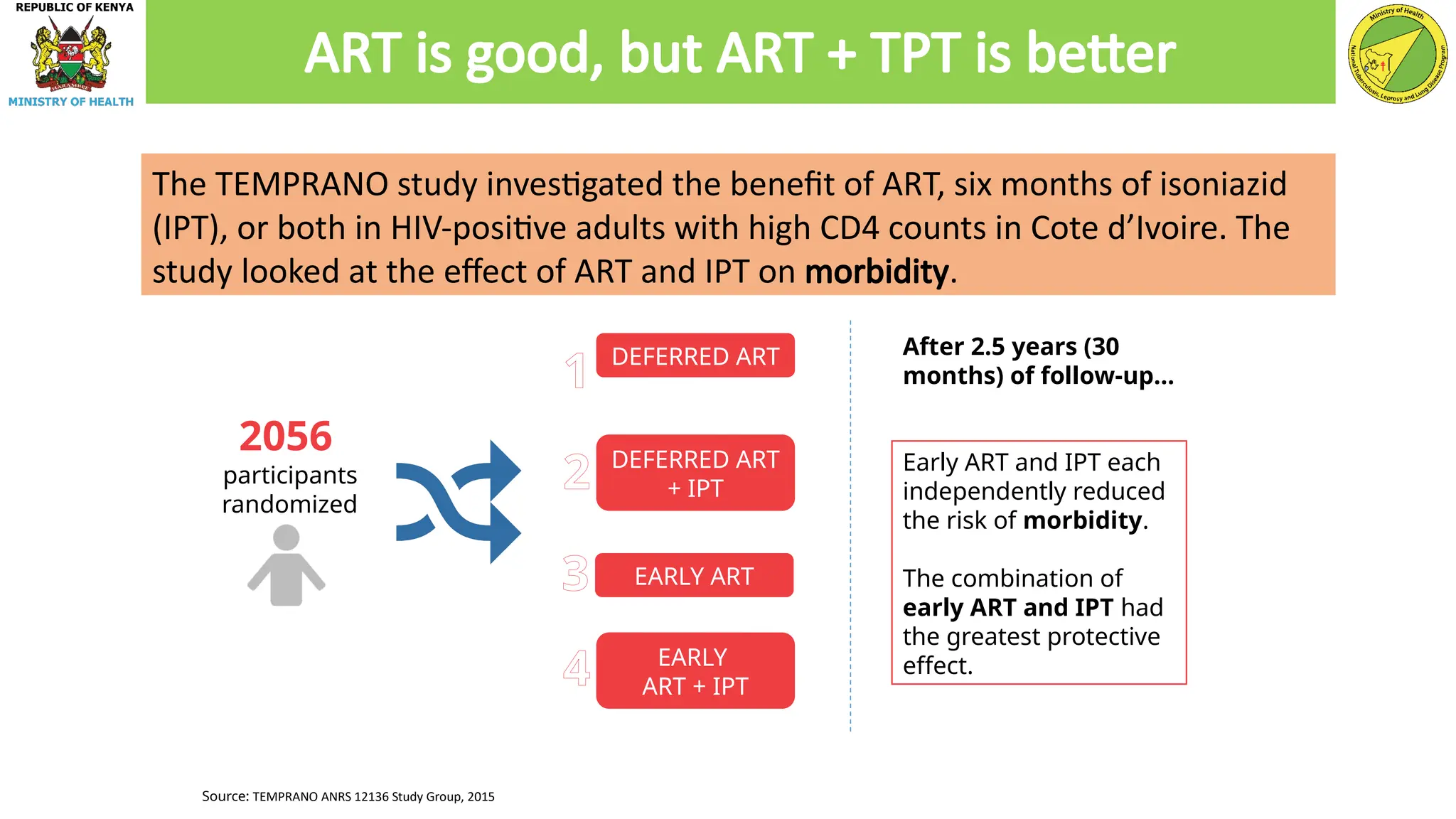
Source: TEMPRANO ANRS12136 Study Group, 2015
2056
participants
randomized
DEFERRED ART
DEFERRED ART
+ IPT
EARLY ART
EARLY
ART + IPT
After 2.5 years (30
months) of follow-up…
1
2
3
4
Early ART and IPT each
independently reduced
the risk of morbidity.
The combination of
early ART and IPT had
the greatest protective
effect.
The TEMPRANO study investigated the benefit of ART, six months of isoniazid
(IPT), or both in HIV-positive adults with high CD4 counts in Cote d’Ivoire. The
study looked at the effect of ART and IPT on morbidity.
ART is good, but ART + TPT is better
12.
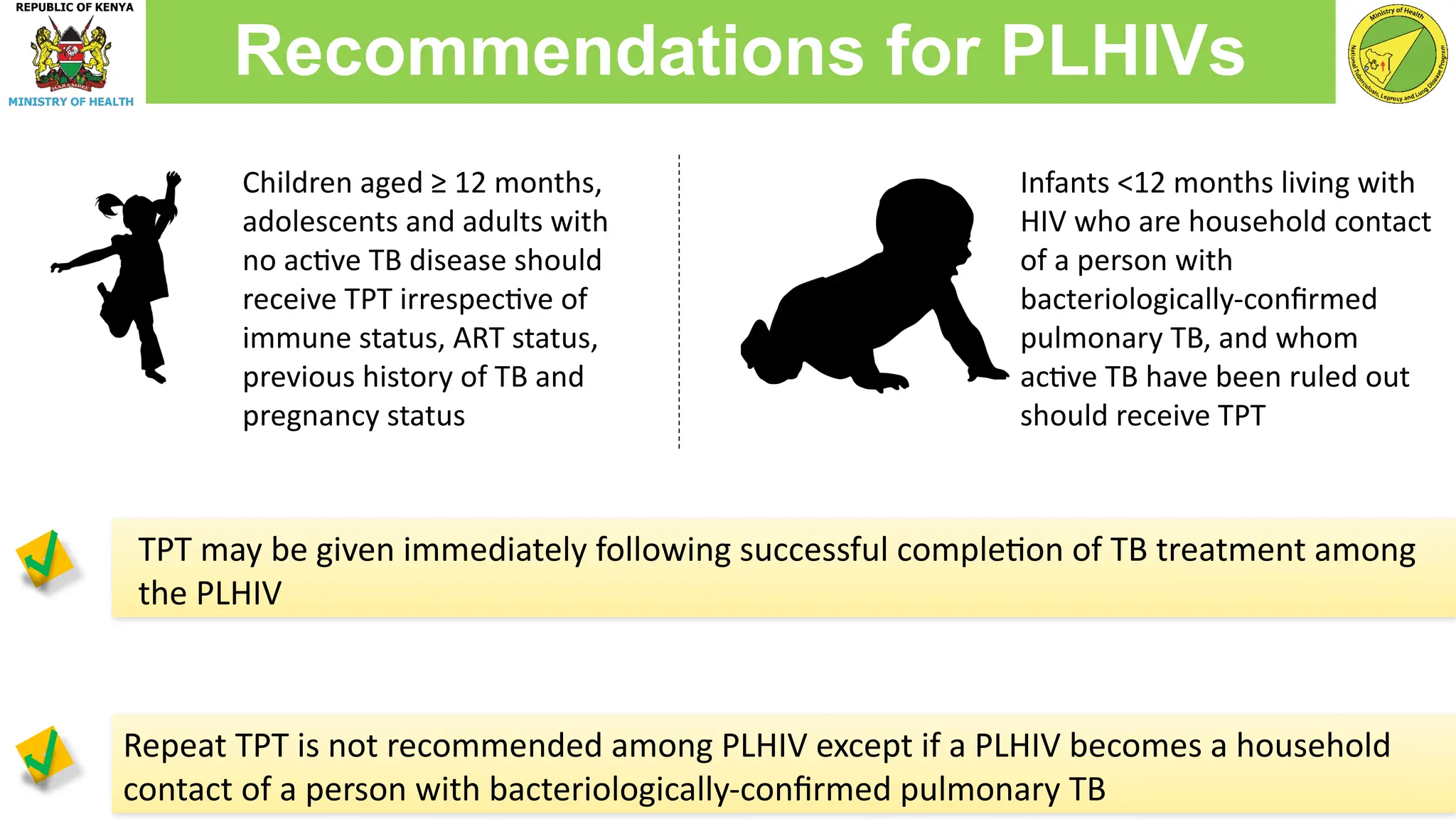
Repeat TPT isnot recommended among PLHIV except if a PLHIV becomes a household
contact of a person with bacteriologically-confirmed pulmonary TB
Recommendations for PLHIVs
Children aged ≥ 12 months,
adolescents and adults with
no active TB disease should
receive TPT irrespective of
immune status, ART status,
previous history of TB and
pregnancy status
Infants <12 months living with
HIV who are household contact
of a person with
bacteriologically-confirmed
pulmonary TB, and whom
active TB have been ruled out
should receive TPT
TPT may be given immediately following successful completion of TB treatment among
the PLHIV
13.
● Prevalence ofLTBI is higher among persons above 5 years of age compared to
children below 5 years
● Children below 5 years are at a higher risk of progression to active TB disease
● Household contacts, regardless of their age have a significantly higher risk of
progression to TB disease compared to general population
● They should be provided with TPT after ruling out active TB disease regardless of
their age and HIV status
NB- Currently, contacts of DRTB patients are excluded from TPT
Household contacts of Bact. confirmed TB cases
14.
1
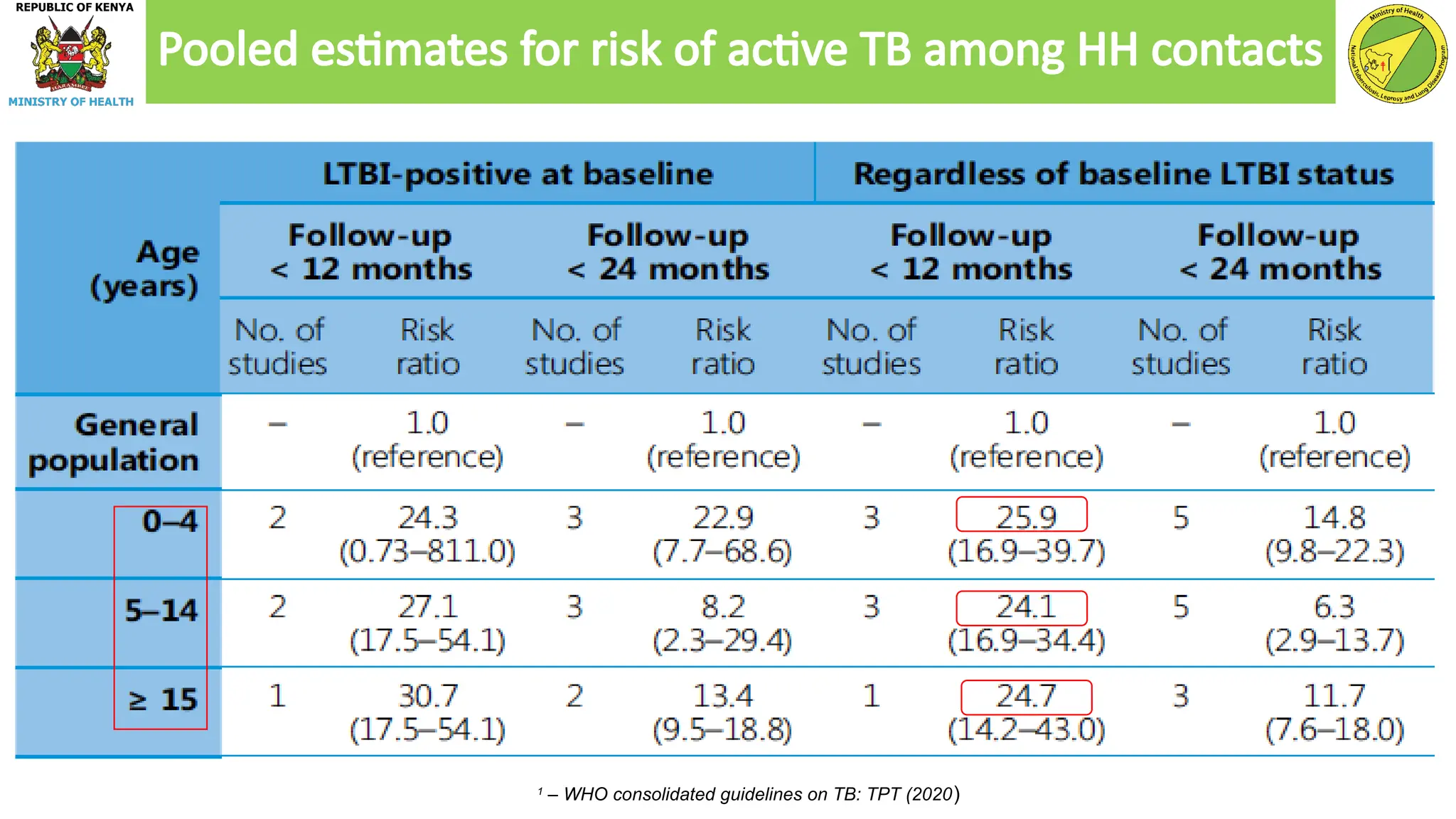
– WHO consolidatedguidelines on TB: TPT (2020)
Pooled estimates for risk of active TB among HH contacts
15.
● All householdcontacts (adults, adolescents and children) of bacteriologically
confirmed PTB should be given TPT after ruling out active TB disease irrespective of
age or HIV status
● Active TB should be ruled out after appropriate clinical evaluation in accordance with
the National guidelines
● Where available, LTBI test (TST or IGRA) may be provided to Adults, adolescents and
children aged ≥5 contacts as part of screening before initiation of TPT
Recommendations for Household contacts
16.
● Global riskof TB in prison is estimated to be 23 times higher than in the general
population
● Risk factors in TB transmission include late diagnosis, inadequate treatment,
overcrowding, poor ventilation and repeated prison transfers
● HIV infection, malnutrition and substance abuse encourage the progression of Latent
TB to active disease
● Due to constant interaction with the prisoners, staff working in prison settings are
also at an increased risk of TB infection
Prisoners and staff working in prison settings
17.
● Prisoners shouldbe screened for TB at entry to prison and thereafter bi-annually
during imprisonment
● TPT should only be given to those who are to be confined for at least 3 months (to
ensure completion
● Staff working in prison settings should also be routinely screened for active TB every
6 months
● Those without active TB disease should be put on a course of TPT (once in their
lifetime)
Recommendations for Prisoners and staff
18.
● Healthcare workersface a two- to three-fold increased risk of developing TB
compared with the general population
● This is due to frequent and prolonged exposure to undiagnosed persons with TB or
DRTB in the workplace
● The increased risk is also attributed to close contact with TB patients and handling of
TB specimens
Health workers and staff in healthcare settings
19.
● HCWs shouldbe regularly screened for TB (at least bi-annually) and adhere to
infection prevention and control measures
● HCWs should be given TB preventive therapy after ruling out active TB disease
irrespective of age or HIV status
Recommendations for health care workers
20.
● Other clinicalat risk groups include;
• Patients initiating chemotherapy or those who are taking certain immunosuppressive
drugs
• Patients receiving dialysis
• Patients preparing for an organ or hematological transplant
• Patients with silicosis
● Patients with weakened immune systems have an increased risk of activating LTBI
and acquiring of TB infection leading to TB disease
● TPT to these patients is essential to prevent progression to disease
Other populations at risk
21.
Due to lackof strong evidence TPT is not recommended for the following unless
they belong to other risk groups;
1. Persons with diabetes
2. Those who inject drugs
3. Those with harmful alcohol use
4. Tobacco smokers
5. The homeless
6. Malnourished
7. Immigrants from high TB burden countries
Unless they meet the criteria for TPT target populations
Populations excluded from TPT
22.
Symptomatic screening shouldbe conducted to all at-risk populations
TPT should be offered to the asymptomatic individuals
Those with symptoms should be offered TB diagnostics investigations and managed
appropriately
TB cardinal symptoms
• Children: Persistent cough, Fever , Poor feeding, Weight loss/failure to thrive,
Fatigue, Reduced playfulness and decreased activity
• Adults: Cough, Night sweats, Fever, Weight loss
Note: Testing using TST or IGRA where available could be offered to the asymptomatic before initiating TPT
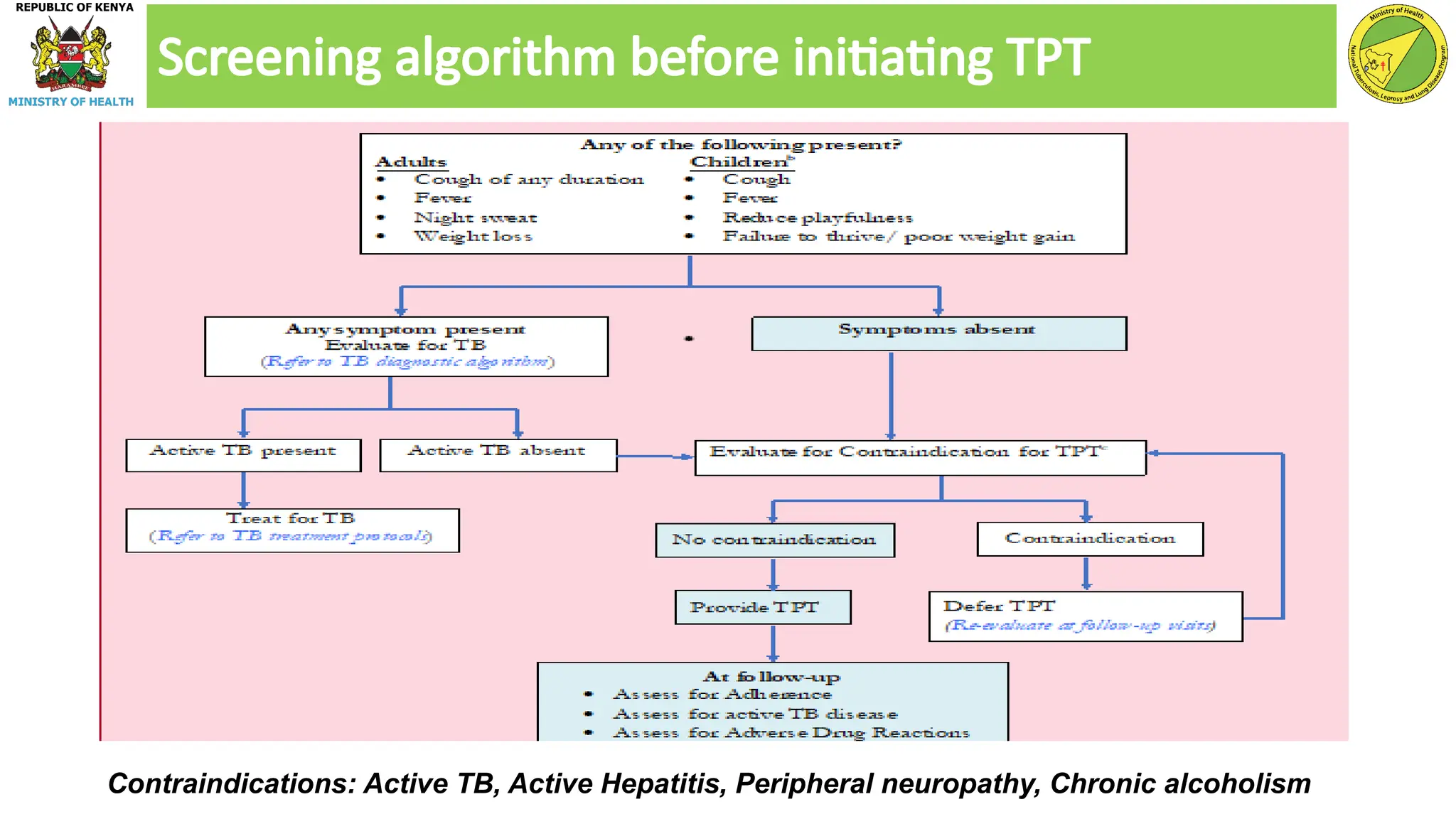
LTBI screening Algorithm
23.
Screening algorithm beforeinitiating TPT
Contraindications: Active TB, Active Hepatitis, Peripheral neuropathy, Chronic alcoholism
24.
Discussion session
What aresome of the strategies we can put in place to ensure that the following
populations are identified, screened for TB and offered TPT?
1. PLHIVs
2. HCWs
3. Household contacts of pulmonary Bact. Confirmed TB patients
4. Prisoner and those in prison settings
5. Clinical risk groups
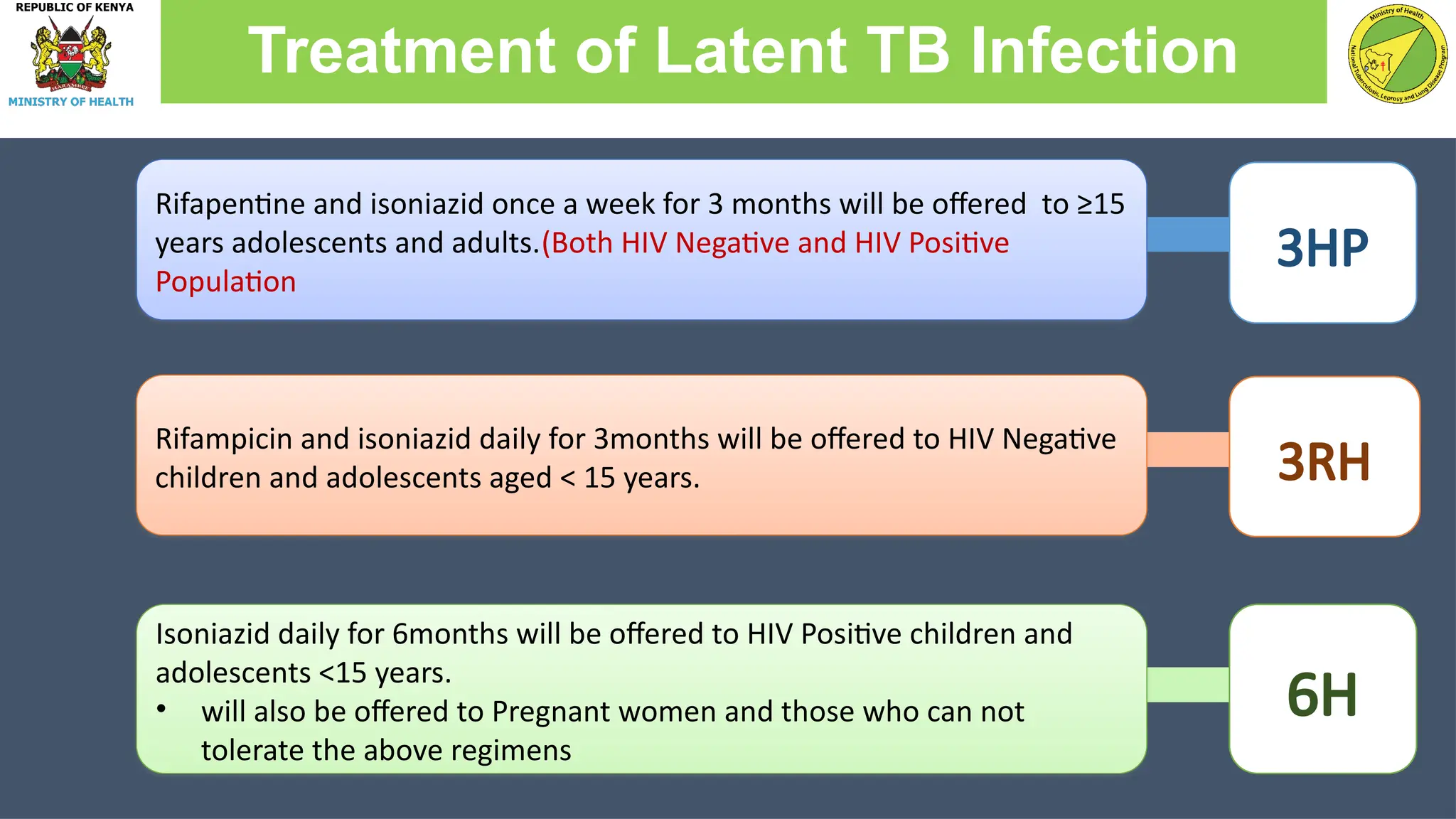
3HP
Treatment of LatentTB Infection
Rifapentine and isoniazid once a week for 3 months will be offered to ≥15
years adolescents and adults.(Both HIV Negative and HIV Positive
Population
Rifampicin and isoniazid daily for 3months will be offered to HIV Negative
children and adolescents aged < 15 years. 3RH
Isoniazid daily for 6months will be offered to HIV Positive children and
adolescents <15 years.
• will also be offered to Pregnant women and those who can not
tolerate the above regimens
6H
27.
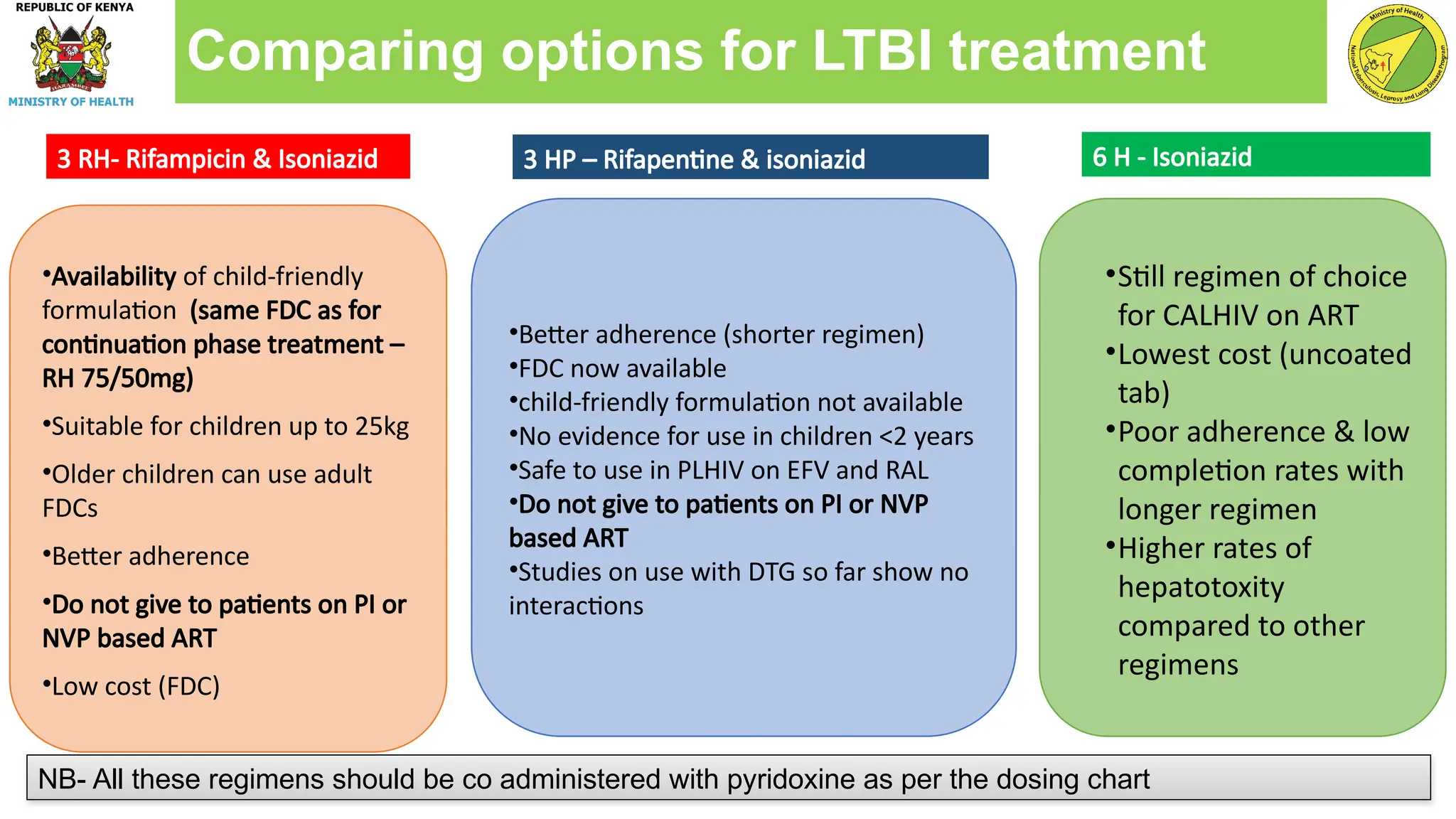
•Availability of child-friendly
formulation(same FDC as for
continuation phase treatment –
RH 75/50mg)
•Suitable for children up to 25kg
•Older children can use adult
FDCs
•Better adherence
•Do not give to patients on PI or
NVP based ART
•Low cost (FDC)
•Better adherence (shorter regimen)
•FDC now available
•child-friendly formulation not available
•No evidence for use in children <2 years
•Safe to use in PLHIV on EFV and RAL
•Do not give to patients on PI or NVP
based ART
•Studies on use with DTG so far show no
interactions
•Still regimen of choice
for CALHIV on ART
•Lowest cost (uncoated
tab)
•Poor adherence & low
completion rates with
longer regimen
•Higher rates of
hepatotoxity
compared to other
regimens
NB- All these regimens should be co administered with pyridoxine as per the dosing chart
6 H - Isoniazid
3 HP – Rifapentine & isoniazid
3 RH- Rifampicin & Isoniazid
Comparing options for LTBI treatment
28.
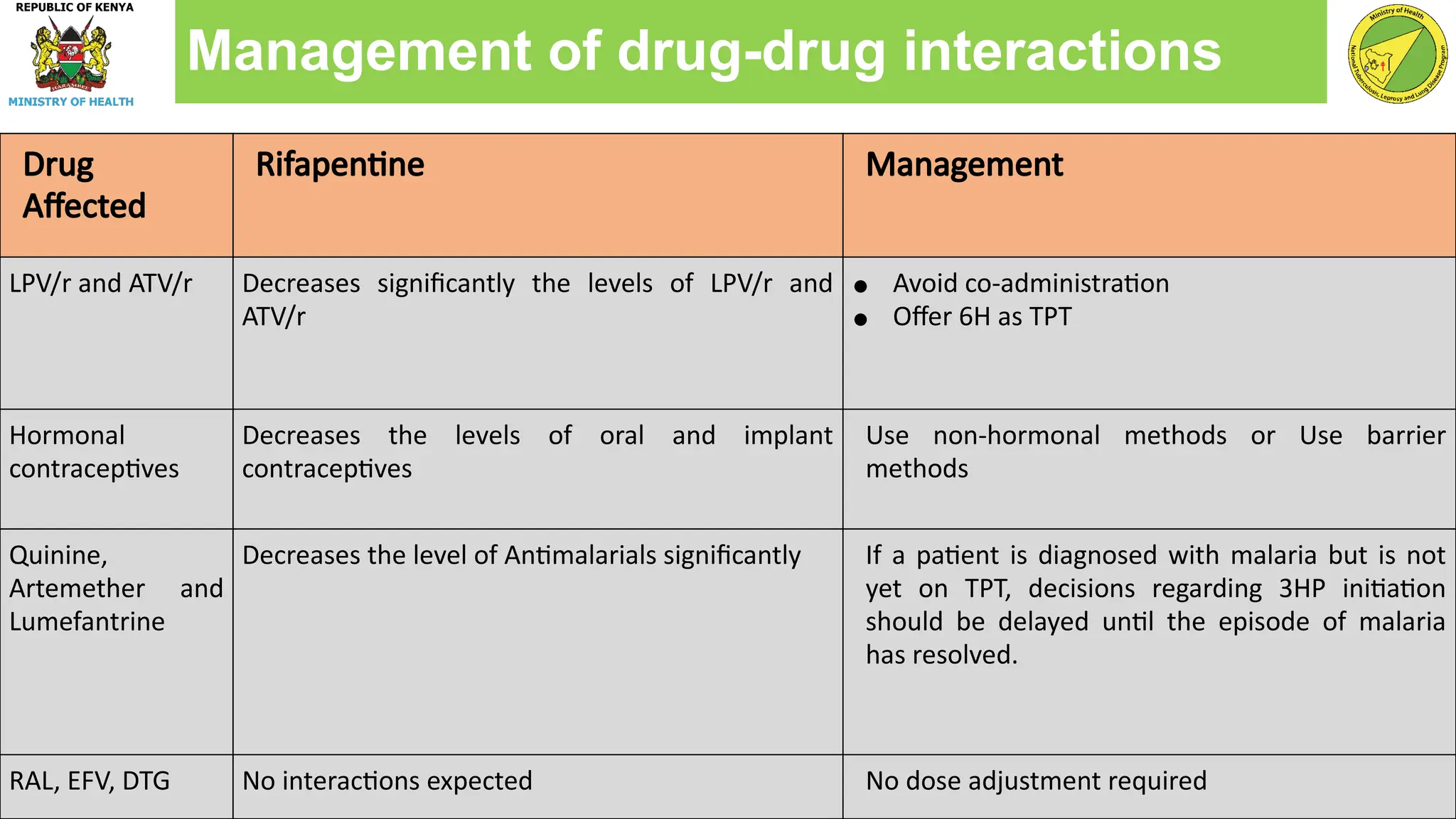
Drug
Affected
Rifapentine Management
LPV/r andATV/r Decreases significantly the levels of LPV/r and
ATV/r
● Avoid co-administration
● Offer 6H as TPT
Hormonal
contraceptives
Decreases the levels of oral and implant
contraceptives
Use non-hormonal methods or Use barrier
methods
Quinine,
Artemether and
Lumefantrine
Decreases the level of Antimalarials significantly If a patient is diagnosed with malaria but is not
yet on TPT, decisions regarding 3HP initiation
should be delayed until the episode of malaria
has resolved.
RAL, EFV, DTG No interactions expected No dose adjustment required
Management of drug-drug interactions
29.
• Eligible candidatesshould be screened to rule out active TB
Those who screen negative for TB, should be initiated on appropriate TPT regimen
Signs and symptoms of liver disease including yellowness of eyes, abdominal pain should
be ruled out before treatment initiation
Asses for:
• Comorbidities like diabetes mellitus, neuropathy (persistent numbness and burning
sensation in the feet and hand
• Active substance or alcohol use/abuse
Consideration before initiating treatment
30.
Health care workersshould educate the clients on the following:
Reasons for initiating TPT
Importance of adhering to treatment
Signs and symptoms for TB and prompt reporting to the health facility
Ideal nutritional status
Drugs and substance abuse/indigenous medicine
Side effects associated with treatment
Pre- treatment adherence counseling
Non adherence to TPT will end up in progression to active TB or development of drug
31.
Patients on TPTshould be followed up on monthly basis and other clinic
appointments harmonized.
During each clinic visit, conduct the following;
• Symptom based TB screening and update TB status
• Assess and reinforce adherence of the patients to ascertain compliance and
completion of doses
• Assess for any adverse drug reactions and intervene appropriately
Follow Up of Patients on TB preventive therapy (TPT)
If a patient screens positive for TB while on TPT, stop TPT and manage according to National
32.
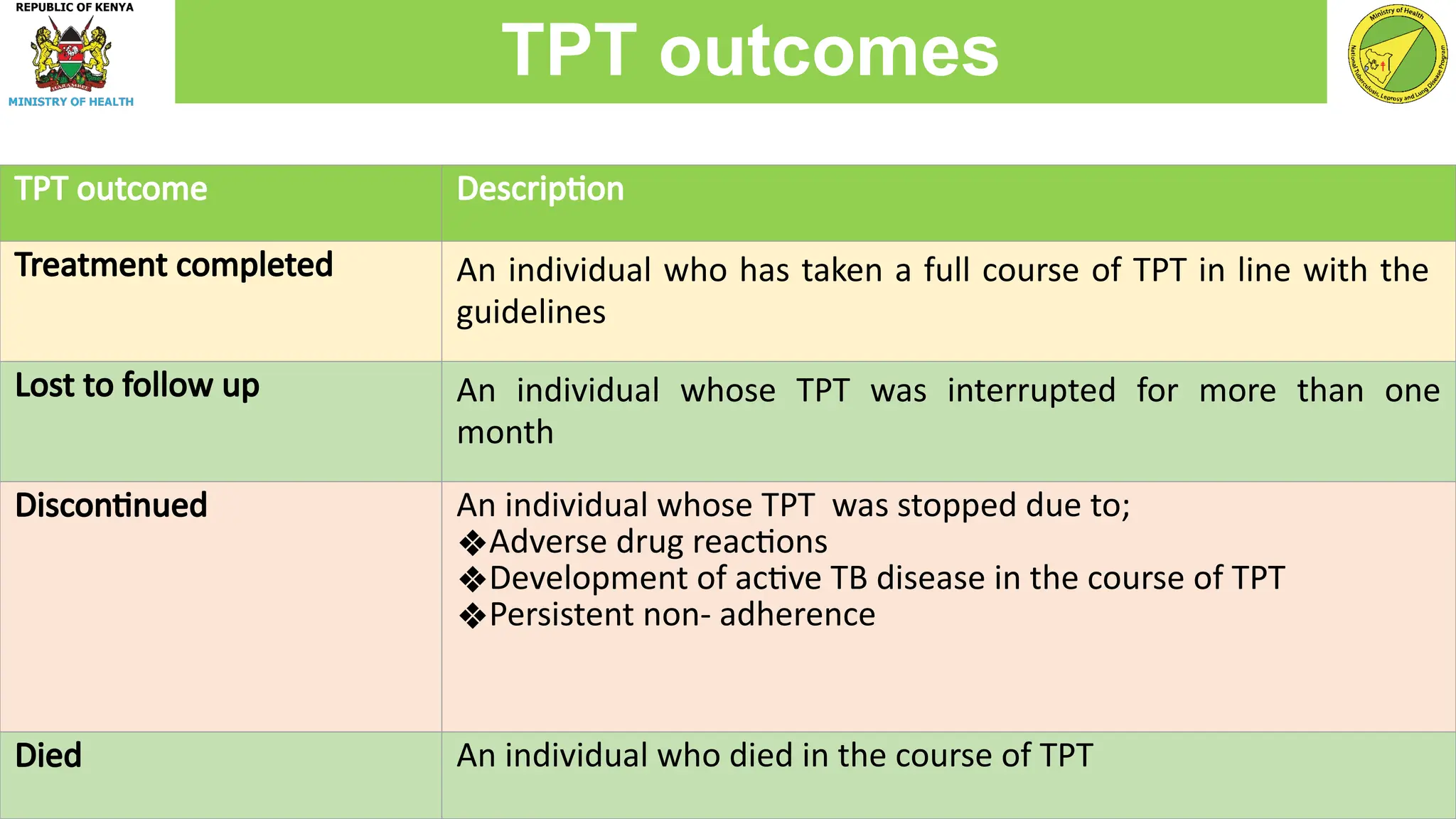
TPT outcome Description
Treatmentcompleted An individual who has taken a full course of TPT in line with the
guidelines
Lost to follow up An individual whose TPT was interrupted for more than one
month
Discontinued An individual whose TPT was stopped due to;
❖Adverse drug reactions
❖Development of active TB disease in the course of TPT
❖Persistent non- adherence
Died An individual who died in the course of TPT
TPT outcomes
33.
Conduct symptom-based TBscreening
• At every clinic visit for PLHIVs
• At month 6 and month 12 for the HIV negative clients
If a patient screens positive after completing TPT, manage according to national TB
guidelines
Follow up after completion of TPT
34.
You are workingin a TB clinic and have recently learned about the importance of
child contact management.
You know from previous data that on average, you will identify 1 child under 5
years of age for every 3 index cases
In the past 6 months, there have been 300 bacteriologically positive index cases
and 50 child contacts recorded in the child contact register. Of these, 45 have
come in for screening, 2 were diagnosed with active TB disease. 40 were initiated
on TPT and 38 had documented completion. Where are most of the losses
happening? What are some strategies to help you confirm?
Case study 1
35.
Suspect child contactidentification challenges if number of child contacts identified
is lower than average child contacts < 5 years/adult
What do you do?
• You could consider consider randomly sampling bacteriologically-positive index
cases and conducting household visits. Does the number of child contacts
during visit match what was reported?
• Are healthcare workers having difficulty documenting child contacts?
• Are index cases understanding the question?
Case study 1 Cont’d..
36.
You have improvedyour identification strategy by providing HCW education. You review
your data again six months later and there have been 250 bacteriologically positive index
cases and 150 child contacts recorded in the register. 75 have come in for screening, 5
were diagnosed with active TB disease. 68 were initiated on PT and 68 had documented
completion.
Where are the losses occurring? What else do you want to know? What are some possible
solutions?
Case study 2
37.
• Healthcare workersreport that with the increased number of children identified, it
has been very difficult to keep up with managing the active cases and conducting
child contact management.
• Possible Solutions
• Assign one day a week (a lighter active TB patient day) to child contact
management screening and ask index cases to bring children on that day
• Remember, chest x-ray is not necessary – if asymptomatic and machine is down
or other issues, START PT
Case study 2 cont’d..
38.
You decided todedicate one day a week to child contact management and you have
one staff member who is in charge of doing the screening on that day. This is working
well and you are screening >90% of child contacts identified.
You learn that index cases have been asking to transfer their child contacts to a TB
clinic that is closer so although there is documentation that IPT was recommended,
50% of the asymptomatic child contacts were labeled ‘transferred out’ and no IPT was
initiated.
How do you handle this?
What strategies could you think of to over come this challenge?
Case study 3
39.
• Transfer challenges
•Can give child contacts initial dose of IPT and document in register. HCWs can then
make follow up call to transfer facility to assess completion.
• Stigma challenges
• There may be stigma against TPT amongst healthcare workers and the community.
Educate, educate, educate!
• Ask about disclosure
Case study 3 cont’d..
40.
Zawadi is an8 year old female, lives in Thika, identified through contact tracing. Her
father who is a banker recently tested Positive for TB, sputum smear +, MTB detected,
Rif sensitive.
HIV Testing done and was Negative
She is a grade 2 pupil and currently on break because of the COVID 19 Pandemic
•What plan will you give Zawadi?
•What TPT Regimen will you consider for Zawadi?
•How differently will you treat Zawadi if she was HIV Positive?
Case study 4
41.
46 year oldmale, born in Murang’a, history of homelessness in the last 5 years,
excessive drug and alcohol use but stopped one year ago. CXR: Left upper lobe
consolidation and left hilar lymphadenopathy, GENE XPERT- MTB detected, Rif
Sensitive. Newly diagnosed HIV POSITIVE
•What do we do for this patient?
•When do we initiate ART?
•When do we start TPT?
•What TPT regimen do we start this client on?
Case study 5
42.
Salim is a42 year old Male, Currently serving a 6 months jail term at
Kiambu Maximum Prison. Presents with no symptom suggestive of Active
TB disease.
•Does Salim qualify for TPT?
•What Regimen will you give Salim?
Case study 6
Editor's Notes
#2 Most infected people have no signs or symptoms of TB but are at risk for active TB disease
Also referred to as LTBI treatment or preventive therapy
#4 the risk for active TB disease after infection depends on several factors, the most important being immunological status
TPT can offer protection for up to 5 years after initial infection.
#14 TPT after completion of treatment gives additional protective benefit by eliminating any dormant bacilli that were not killed by anti-TB treatment
#16 The prevalence of LTBI was higher among children and adolescents aged > 15 years and adults than in children < 5 years, who were at greatest risk for progression to active TB disease.
All household contacts, regardless of their age or LTBI status, were at a substantially higher risk for progression to active TB than the general population
#17 Appropriate clinical evaluation should include assessment of the intensity of and risk for exposure, the risk for development of active TB and/or ascertainment of infection by testing for LTBI.
#20 For the purposes of TB prevention in Kenya, the definition of health care workers extends beyond those frequently engaged in direct clinical and nursing care to include even those in administrative and clerical duties. It also includes students who are in their clinical years or interact with patients frequently. This broad definition thus includes, and not limited to, doctors (including those in administrative roles), clinical officers, nurses, laboratory technologists, community health workers, students (especially those in clinical years), paramedical staff (e.g., public health officers, physiotherapists, community health volunteers, occupational therapists), support staff (including clerical officers, casual workers, drivers, receptionists, telephone operators) among others.
#30 On hormonal contraceptives need further discusions
#31 Explain to participants how to assess for DM, nutrition, neuropathy, alcohol use
#32 Facilitator to discuss with the participants each of the points above
#33 PLHIVS on TPT do not put under the stable patients category