ANATOMY OF SYSTEMINVOLVED IN
OXYGENATION PROCESS
• The main organs involved in process of oxygenation
are heart and lungs .Blood from all the body parts
enters to the heart through superior and inferior vena
cava to right atrium .During atrial systole the blood is
ejected to right ventricle through tricuspid valve .From
right ventricle ,pulmonary artery takes blood to lungs
for oxygenation and oxygenated blood returns to left
atrium and then ventricle via pulmonary vein .Left
ventricle then supplies oxygenated blood to whole
body via arteries .
3.
PROCESSOF RESPIRATION
• Airenters through nose ,where it is warmed ,humidified and filtered
• Inspired air passes from the nose through the pharynx
• After this air moves to trachea passing through larynx
• Trachea branches into two bronchi supplying right and left lungs
• Through bronchi air enters into lungs and moves through primary
bronchi ,smaller and capillary walls from respiratory membrane where the
gas exchange occurs
4.
PHYSIOLOGY OF RESPIRATION
•PULMONARY VENTILATION - This means movement of air into and out of
the lungs .Its main purpose is to supply fresh air
• Ventilations is composed of ;
o INSPIRATION-When airflows into the lungs
o EXPIRATION-When air moves out of the lungs
Adequate ventilation depends upon,
1. Clean airways
2. An intact central nervous system and respiratory centre
3. An intact thoracic cavity capable of expanding and contracting
4. Adequate pulmonary compliance and recoil
5.
OXYGEN
Oxygen is acolorless , odorless ,tasteless gas
which can assist patients in a variety of
circumstances and is universally accepted for
routine use in hospital settings .Oxygen
constitutes 88.8% of the water and 20.9%of the
volume of air .
6.
.
DEFINITION
Oxygenation is theprocess that includes both the inspiratory
and expiratory activities hence there occurs the exchange or
transport of respiratory gases
Oxygen therapy is the administration of oxygen as a therapeutic
modality
Oxygen therapy benefits the patient by increasing the supply of
oxygen to the lungs and thereby increasing the availability of
oxygen to the body tissues
7.
FACTORS AFFECTING RESPIRATORY
FUNCTIONING
PAIN– Pain alters rate and rhythm of
respiration .patient inhibits chest wall movement while
experiencing pain in chest or abdomen .
EXERCISE –Exercise increases rate and depth of
respiration to meet the bodys need for additional
oxygen .
8.
.
Emotions: Some strongemotions, such as
fear, anger and nervousness can stimulate
respiratory centre,resulting in respiration pause
or increased rate of respirations. Anxiety
increases rate and depth as a result of
sympathetic stimulation.
Body posture: A straight, erect posture
promotes full chest expansion and lying flat
prevents full chest expansion.
9.
. Neurological injury:Injury to brainstem impairs
respiratory centre and inhibits respiratory rate and
rhythm.
Medication: Narcotic analgesics and sedatives
depress rate and depth. Amphetamines and cocaine
may increase rate and depth of respiration.
Blood pressure: Blood pressure can influence
respiration when it fluctuates in a large range. If the
blood pressure increases, the respiration will decrease
in rate and depth.
10.
ALTERATIONS IN RESPIRATORYFUNCTIONING
CONDITIONS AFFECTING AIRWAY
ALLERGIES
oDefinition –It occurs when immune system
responds to foreign particle like
pollen ,dust ,any food ,etc.
oSymptoms –sneezing ,running and stuffy
nose ,cough ,chest tightness ,wheezing
sounds
11.
.
ASTHMA
oDefinition-It is characterizedby
inflammation ,bronchospasm and edema
of the airway
oSymptoms –Coughing ,shortness of breath
,cyanosis ,anxiety ,rapid pulse ,chest
tightness
12.
.
BRONCHITIS
oDefinition-It is aninflammation of the
bronchial tubes that carry airto the lungs.
oSymptoms- Cough, Mucus production,
Shortness of breath, Chest tightness, Low
grade fever
13.
. COUGH
oDefinition-. Itis the forceful expulsion of respiratory
content. It is the body's response when something
irritates in throat or airways. An irritant stimulate the
nerves that send a message to brain. The brain then send
message to muscles of chest and abdomen to push air
out of lungs to force out the irritant. Hardly cough is
normal and healthy. A cough that persists for several
weeks or one that brings up discolored or bloody mucus
may indicate a condition that needs medical attention.
14.
.
oCauses-
Airways irritants(smoke ,pollen,dust,foreignbody),
parenchymal lung diseases –
pneumonia ,TB,COPD ,Whooping cough ,acute sinusitis
(nasal and sinus infection),corona virus disease 2019
oSymptoms- Fever, Purulent postnasal discharge ,
Increased malaise, Dyspnea or localized pain,
Productive cough with expectoration of
purulentmaterial, sore throat, Wheezing and shortness
of breath ,Heartburn or a sour taste in your
mouth ,Rarely, coughing up blood.
15.
. TYPES OFCOUGH
There are two types of cough:
According to Severity
1. Acute cough: It occurs due to irritation of
trachea and it has sudden onset.
2. 2. Chronic cough: It occurs in any disease
condition likeTB, asthma, COPD, etc
16.
CONDITIONS AFFECTING MOVEMENTOF AIRWAY
DYSPNEA
Definition- It is defined as the sensation of
breathlessness or inadequate breathing. It is the
abnormal uncomfortable awareness of breathing.
Dyspnea, also called shortness of breath, is a
tight feeling in chest in which person may not be
able to take a deep breath. This is a symptom
that can be connected to many different
conditions, like asthma, heart failure and lung
disease.
17.
. GRADING
Grade-Dyspnea occurs while doing strenuous
activities.
Grade 2: Person is restricted to some activities like
climbing stairs.
Grade 3 -Dyspnea occurs during usual activities but
person can manage.
Grade 4: Person requires assistance while performing
activities of daily living
Grade 5: Dyspnea occurs at rest.
18.
.
oCAUSES-
Anemia ,asthma ,anxiety,heart or lungs
problems like heartfailure ,COPD etc ,history of
smoking ,severe obesity ,allergic reactions ,injury
to the ribs,exposure to dangerous level of
carbonmonoxide gas .
oSYMPTOMS-
Shortness of breath,feeling of
suffocation ,chest tightness ,chest pain .breathing
difficulty ,blue finger or lips ,swelling in ankles and
feets .
19.
. TACHYPNEA
oDEFINITION- Itis defined as when respiratory
rate is more than 24 breath per minute
oCAUSES-Exercise ,heavy physical
activity ,anxiety allergic reactions ,foreign body
aspiration
20.
. oSYMPTOMS-Feeling ofshortness of breath ,confusion ,sweating
,high body temperature
BRADYPNEA
oDEFINITION –when the respiratory rate less than 16 breaths per
minute
oCAUSES-Opiods overload ,smoking ,alcoholism ,lungs diseases
like COPD ,Asthma ,hypothyroidism ,head injury ,use of
sedatives and anesthesia ,exposure to carbonmonoxide gas.
oSYMPTOMS –Decrease alertness,itching ,dry
skin ,headache ,weakness ,dizziness ,,cyanosis ,loss of
consciousness .
21.
ORTHOPNEA
oDEFINITION –It isdefines as shortness of breath
when the patient is lying down
oCAUSES-heartdisease,pneumonia ,obesity ,paralysis
of diaphragm
oSYMPTOMS –shortness of breath ,chest tightness
22.
.
APNEA
oDEFINITION- It isthe cessation of
breathing in which there is no movement of
respiratory muscles for inhalation and
expiration and the volume of the lungs
remain unchanged.
23.
. SLEEP APNEA
oDEFINITION-It is the cessation of breathing during sleep.
Types
1. Central sleep apnea: In this apnea brain is unable to send
signals to respiratory muscles for breathing during sleep.
2. Obstructive Sleep Apnea: It is characterized by collapse of
airway during deep sleep.
3. Mixed sleep Apnea: It is the mixture of both central sleep
apnea and obstructive sleep apnea.
24.
.
o CAUSES
Certain drugs,.Choking , Neurological disease ,
Trauma,Emotions , High altitude, Family history,
Reduction in blood oxygen , Narrowed airway,
Hypotonia(decreased muscle tone ), Heart
disease ,Deviated septum.
o SYMPTOMS
Dry mouth ,Headache , Insomnia ,Restless sleep ,Day
time sleepiness, irritability ,poor memory and
attention ,confusion,mood and personality changes.
25.
CONDITIONS AFFECTING DIFFUSION
PULMONARYEDEMA
• DEFINITION -It is defined as an abnormal
accumulation or collection of fluid in lung, lung tissue or
alveolar space. It is a severe and life threatening
condition.
• ETIOLOGY-Sudden, severe hypertension ,MI,
cardiomyopathy , Mitral or aortic valve disorder Major
injury, Lung damage caused by poisonous gas or
severe infection, Kidney failure
26.
.
• CARDIOGENIC CAUSES– Artherosclerosis ,
Valvular and myopathic disorders , Hypertension ,
Blood blocking up into the pulmonary circulation
cause high pressure ,MI, cardiomyopathy
• Non-cardiogenic Causes - After pneumonectomy ,
Drug over dose and non cardiac pulmonary
edema, Renal failure
27.
.
•CLINICAL MANIFESTATIONS -
Dyspnea,central cyanosis (cyanosis
of lips or nails),anxiety, cough , While
doing suctioning Frothy and blood
mixed .secretions are
seen,Respiratory distress ,irregular
and rapid heart beat .pale skin ,leg
swelling .
28.
.
CHRONIC OBSTRUCTIVE PULMONARY
DISEASES(COPD)
•It is a respiratory disease in which airflow is obstructed
by emphysema(airsacs in the lungs damaged), chronic
bronchitis or both. Asthma is also considered within this
disease group but asthma is reversible.
• Etiology - Passive smoking , Family history ,
Infection ,Lung growth , Bronchitis , Asthma , Air
pollution , Cigarette smoking.
29.
.
• Clinical Manifestations-Chronic coughing
(productive cough) , Dyspnea, Frequent
respiratory infection, Wheezing. Weight loss,
Tachypnea, Pitting edema, Fatigue, Hemoptysis,
Purulent sputum, Weakness
ATELECTASIS
• It is a respiratory disorder characterized by
collapsed lung.It may be chronic or acute.
Atelectasis is the collapse of part or (much less
commonly) all of a lung.
30.
. Etiology
• Atelectasisis caused by blockage of the air
passages(bronchus or bronchioles) or by
pressure on the outside of the lung.
• Risk factors for developing atelectasis include:
Anesthesia ,foreign body in the airway (most
common in children),lung diseases ,prolonged
bedrest with less changes in position ,tumors that
block an airway
31.
.
CLINICAL MANIFESTATIONS
Dyspnea:Rapid and shallow
breathing, Chest pain , Cough , Fever,
Excessive sweating ,Malaise and
weight loss ,Tachypnea,
tachycardia,cyanosis.
32.
. CONDITIONS AFFECTINGOXYGEN TRANSPORT
o HEART FAILURE
Heart failure is the inability of heart to pump the sufficient blood to meet the
needs of tissue for oxygen and nutrient.
o CAUSES
. Pulmonary embolism(blood clot develop in a blood vesselin the body travels
to an artery in the lungand suddenly form blockage of artery); chronic lung
disease, Hemorrhage and anemia , Anesthesia and surgery , Transfusions or
infusions ,Physical and emotional stress ,Excessive sodium intake.
RISK FACTORS– Hypertension , Hyperlipidemia ,Diabetes ,CAD ,Family
history , Smoking , Alcohol consumption of cardiotoxic drugs .
33.
.
HYPOVOLEMIA
Loss of extracellularfluid volume and decreased circulating blood volume.
• Dehydration
• Dehydration occurs when there is not enough fluid in the body, especialy in
the blood (intravascular area). Although ,there are several types of
dehyration.
• Etiology
Long-term nothing by mouth (NPO) status ,Hemorrhage , Profuse
diaphoresis (sweating) , Diarrhea ,Vomiting , Draining abscesses , Severely
draining wounds ,Systemic infection ,Fever ,Frequent enemas ,Diabetes
insipidus (when the body produces toomuch urine )
34.
.
o Clinical Manifestations
Witha rapid fluid loss manifestations of hypovolemia occur rapidly. When loss
of fluid occurs gradually, the patient’s fluid volume may be very low before
symptoms develop
o Mucous Membranes -Dry, may be sticky.
o Neurologic -Anxiety, Restlessness, Possible coma.
o Integumentary System -Diminished skin turgor, Dry skin, Pale, Cool
extremities.
o Cardiovascular System -Tachycardia, Orthostatic hypotension(form of low
BP that happens when standing after sitting or lying down ), Falling
systolic/diastolic pressure , Flat neck vein, Decreased capillary refill,
Decreased hematocrit.
o Potential Complication -Hypovolemic shock
35.
.
.ALTERATIONS OF OXYGENATION
Thealterations of oxygenation indudes:
1. Hypoventilation
2. Hyperventilation
3. Hypoxia
HYPOVENTILATION
Definition - It is the condition when the level of carbon dioxide in body get
higher than oxygen level. It is defined as an increase in partial pressure of
carbondioxide (more than 45mm Hg).
36.
.
CAUSES
High altitude ,medicationsoverdose like
opioids ,benzodiazepines ,sedatives ,,CNS disease like encephalitis ,trauma
etc .,obesity ,chest wall trauma ,sepsis ,lung and airway disease like
asthma ,pneumonia.
SYMPTOMS
Shortness of breath,fatigue ,cyanosis,headache ,restlessness, sleepiness at
day time ,insomnia ,confusion ,abnormal breath sounds ,visual disturbances .
HYPERVENTILATION
It is defined as when the partial pressure of oxygen is more than the partial
pressure of carbondioxide .The amount of carbondioxide is less in blood .
37.
.
• CAUSES
Stress ,depression,anxiety ,anger ,severe pain ,pregnancy ,vigorous
exercise ,high altitude .
SYMPTOMS
Headache ,sweating ,changes in vision ,poor concentration ,chest
tightness ,numbness or tinglng sensations in feet or hands ,muscle spasm .
HYPOXIA
It is a condition in which the body or a region of the body is deprived of
adequate oxygen supply
SIGNS AND SYMPTOMS
Tachypnea ,dyspnea ,hypertension ,anemia ,restlessness ,disorientation ,cyanosis
TYPES OF HYPOXIA
HYPOXIC HYPOXIA –low PaO2(arterial oxygen tension)
38.
.
CIRCULATORY HYPOXIA–Inadequate pumping of the blood from the lungs to
tissues.
HEMIC HYPOXIA –Decreased oxygen carrying capacity as in anemia or carbon
monoxide poisoning .
DEMAND HYPOXIA –increased tissue consumption of oxygen in hypermetabolic
states like fever ,malignant hyperthermia .
HISTOTOXIC HYPOXIA –utilization of oxygen is abnormal such as in cyanide
poisoning there is inability for tissues oxygen available .
39.
MAINTENANCE OF PATENTAIRWAY
• Airway patency is the ability of a person to breathe, with airflow passing to
and from the lungs through the oral and nasal passages. By maintaining an
open airway, air can flow from nose, mouth into lungs. Airway can be
obstructed by foreign body inhalation, allergic ,trauma, head injury,
respiratory tract infection etc
.A. Patency of airway can be managed by
o Provide high fowler/sitting position to expand chest for easing breathing.
o Assist in deep breathing and coughing exercises
o Coughing –it is the most easy method of clearing the throat but person may
not be able to cough properly in case of respiratory muscle
fatigue ,weakness
40.
.
o Use ofpillow for chest support
o Use of incentive spirometery.
o Early ambulation and frequent position change.
B. Other interventions to maintain patent airway are,
o Removal of foreign body by sweeping mouth with finger and ensure not to
push foreign body towards airway.
o Removal of vomit and regurgitation stuff by suctioning
o Airway manoeuver- Head tilt/chin lift, jaw thrust
o Invasive airway management includes oropharyngeal airway,
nasopharyngeal airway and tracheal intubation.
.
ASSESSMENT- current healthproblem ,cough,sputum ,shortness of
breath ,history and physical examination .
PHYSICAL EXAMINATION –Inspection (cyanosis,chest
retractions) , ,palpation ,percussion ,auscultation (breath sounds).
NURSING INTERVENTIONS
o Positioning : semi fowlers or fowlers position
o Oxygen administration ,artificial airways
o Suctioning
o Chest physiotherapy
o Postural drainage (technique that involves laying /sitting in certain in
certain positions to drain secretions from your airways using gravity)
o breathing exercises .
43.
.
oAssess the airwayand optimize airway position (head tilt or chin
lift)as necessary .
oIncentive spirometry
oChest drainage
oEducate about effective coughing method
oIntake and output chart
oDaily weight measurement
oOral care
oBedrest
44.
DOCUMENTATION
o Clinical assessmentand documentation including
cardiovascular ,respiratory and neurological systems .This should be
done at the commencement of each shift and with any change in the
patients condition .
o Change and document oxygen equipment set up at the commencement
of each shift and with any change in the patients condition .
o Hourly checks should be made for the following ;
Oxygen flow rate
• Oxygen saturation
• Patency of tubings .
• Humidifier settings (if being used)
• Patients pulse rate
45.
,
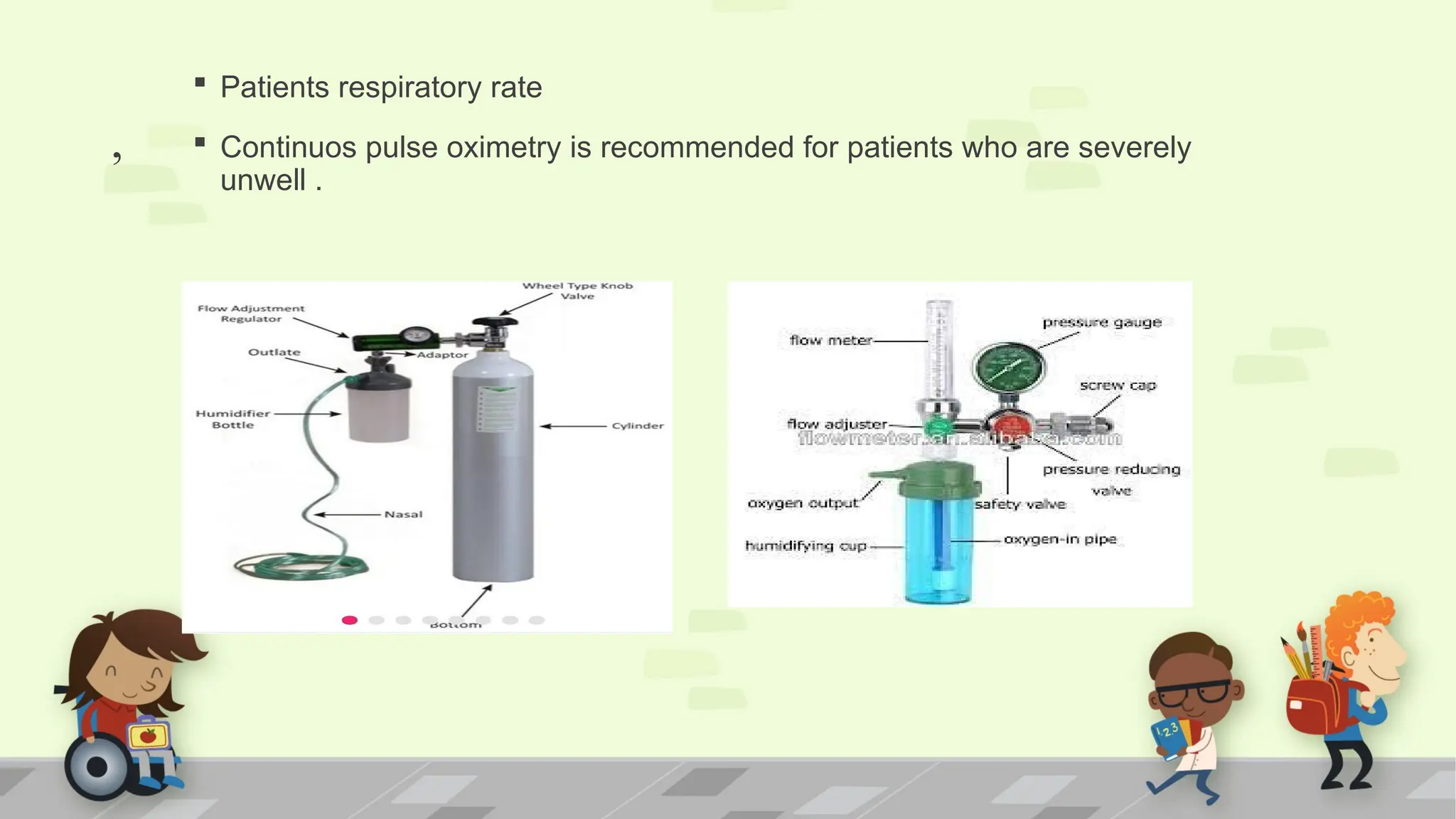
Patients respiratoryrate
Continuos pulse oximetry is recommended for patients who are severely
unwell .
46.
.
INHALATIONS
Inhalation means breathingair or vapor into the lungs through the nose or
mouth .Inhalation is of two types:
1. DRY INHALATION.
2. MOIST INHALATION.
DRY INHALATION
A substance such as ammonia may be inhaled in the treatment of
fainting .
Amyl nitrate may be inhaled to relieve angina
Oxygen inhalation
Inhalation of general anesthetic drugs
Aerosol spray
MOIST INHALATIONS - STAEM INHALATIONS
.
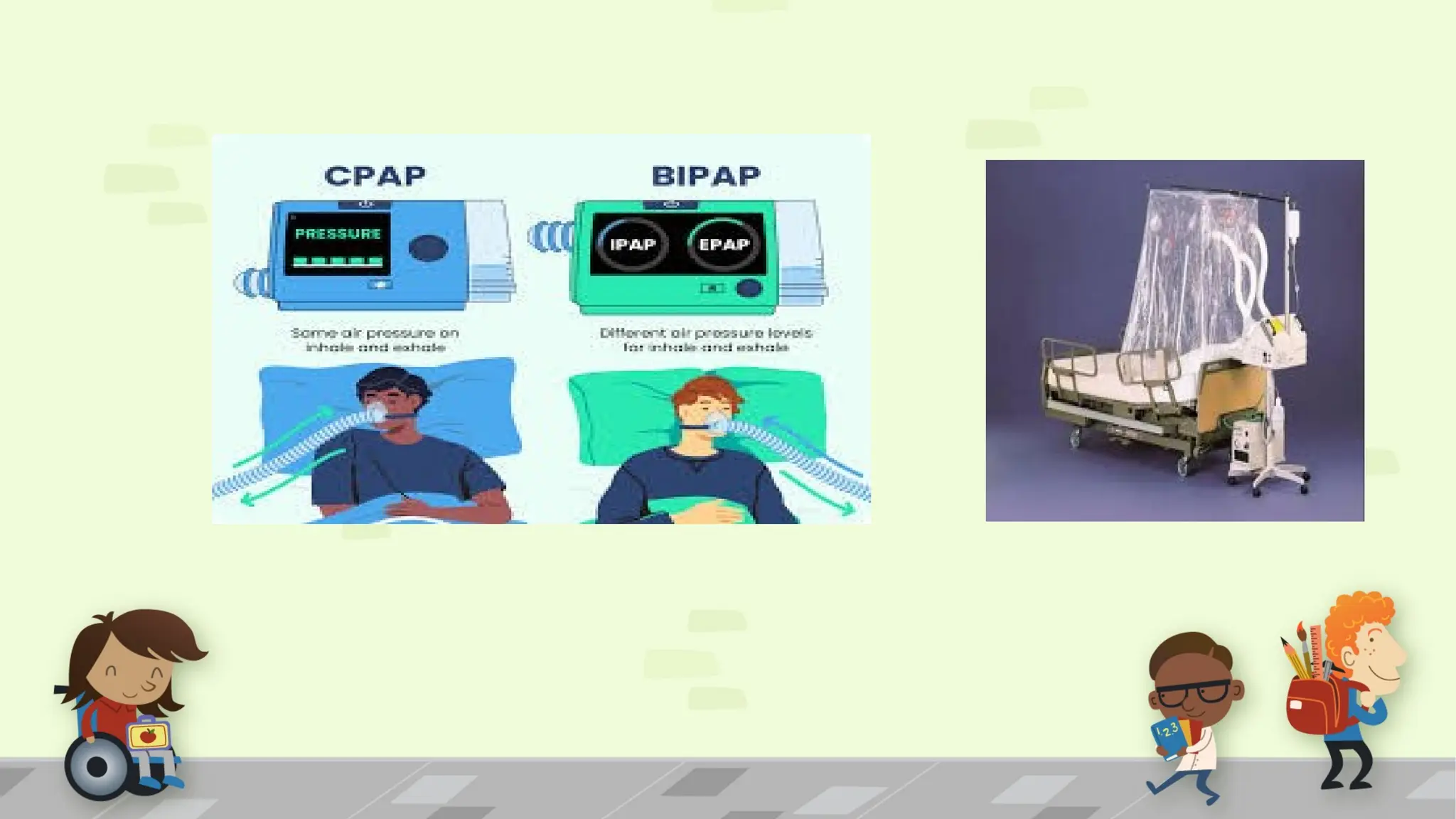
11.BILEVEL POSITIVE AIRWAYPRESSURE (BiPAP)
12.MECHANICAL VENTILATOR
Equipment required for Oxygen Administration
o Patient's chart
o Oxygen connecting tube
o Flow meter
o Humidifier bottle half filled with distilled water
o Oxygen source: Wall Outlets or Oxygen cylinder
o Tray with;
Nasal cannula of appropriate size or Oxygen mask
51.
. Nasal catheterSize-8-14 F the unit of measurement of French
scale (for nasal catheter insertion)
Xylocaine Jelly 2% as lubricant (for nasal catheter insertion)
Kidney tray
Gauze pieces, Cotton swabs – bowl with sterile water
"No smoking" sign board
52.
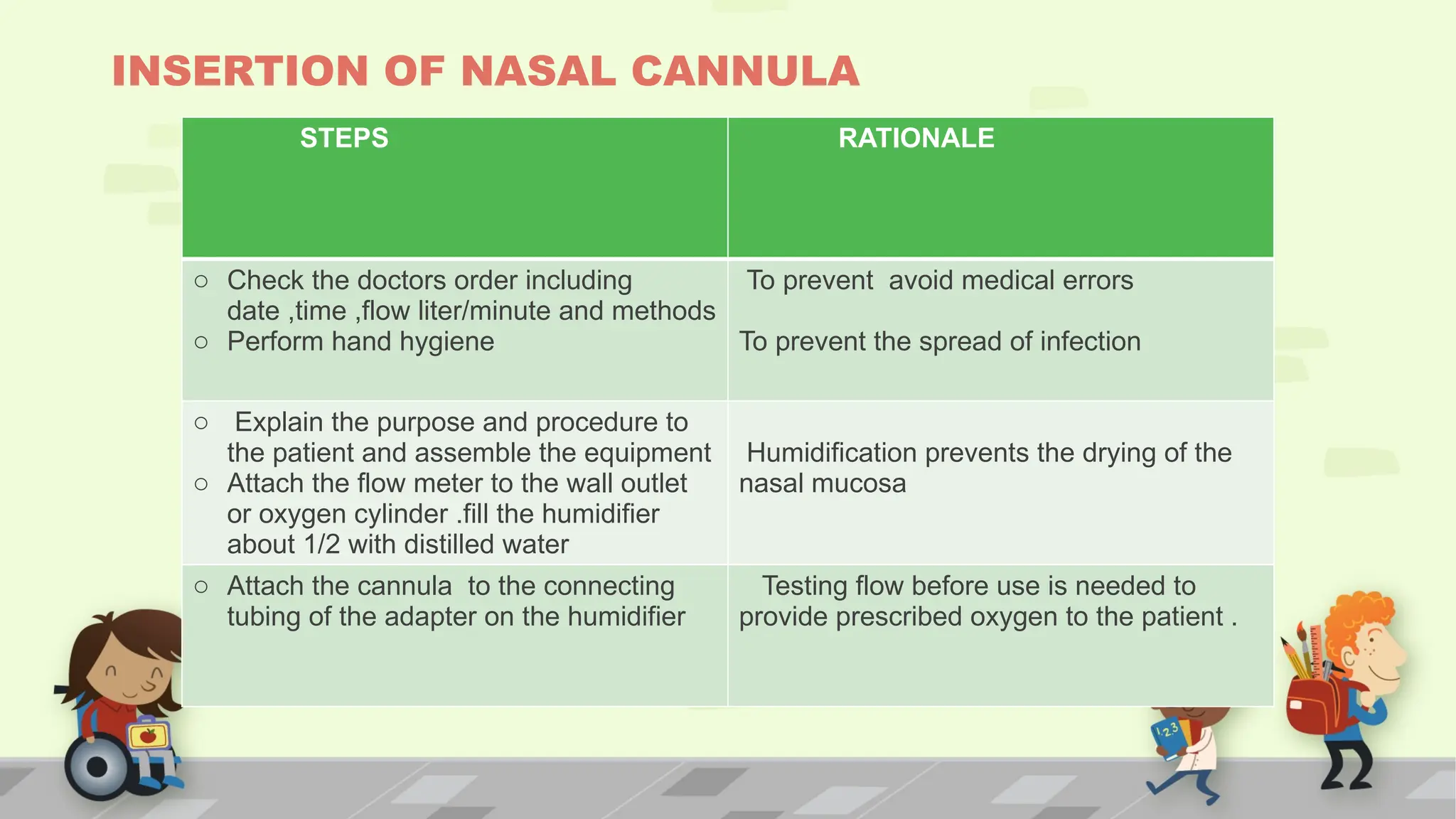
INSERTION OF NASALCANNULA
STEPS RATIONALE
o Check the doctors order including
date ,time ,flow liter/minute and methods
o Perform hand hygiene
To prevent avoid medical errors
To prevent the spread of infection
o Explain the purpose and procedure to
the patient and assemble the equipment
o Attach the flow meter to the wall outlet
or oxygen cylinder .fill the humidifier
about 1/2 with distilled water
Humidification prevents the drying of the
nasal mucosa
o Attach the cannula to the connecting
tubing of the adapter on the humidifier
Testing flow before use is needed to
provide prescribed oxygen to the patient .
53.
.
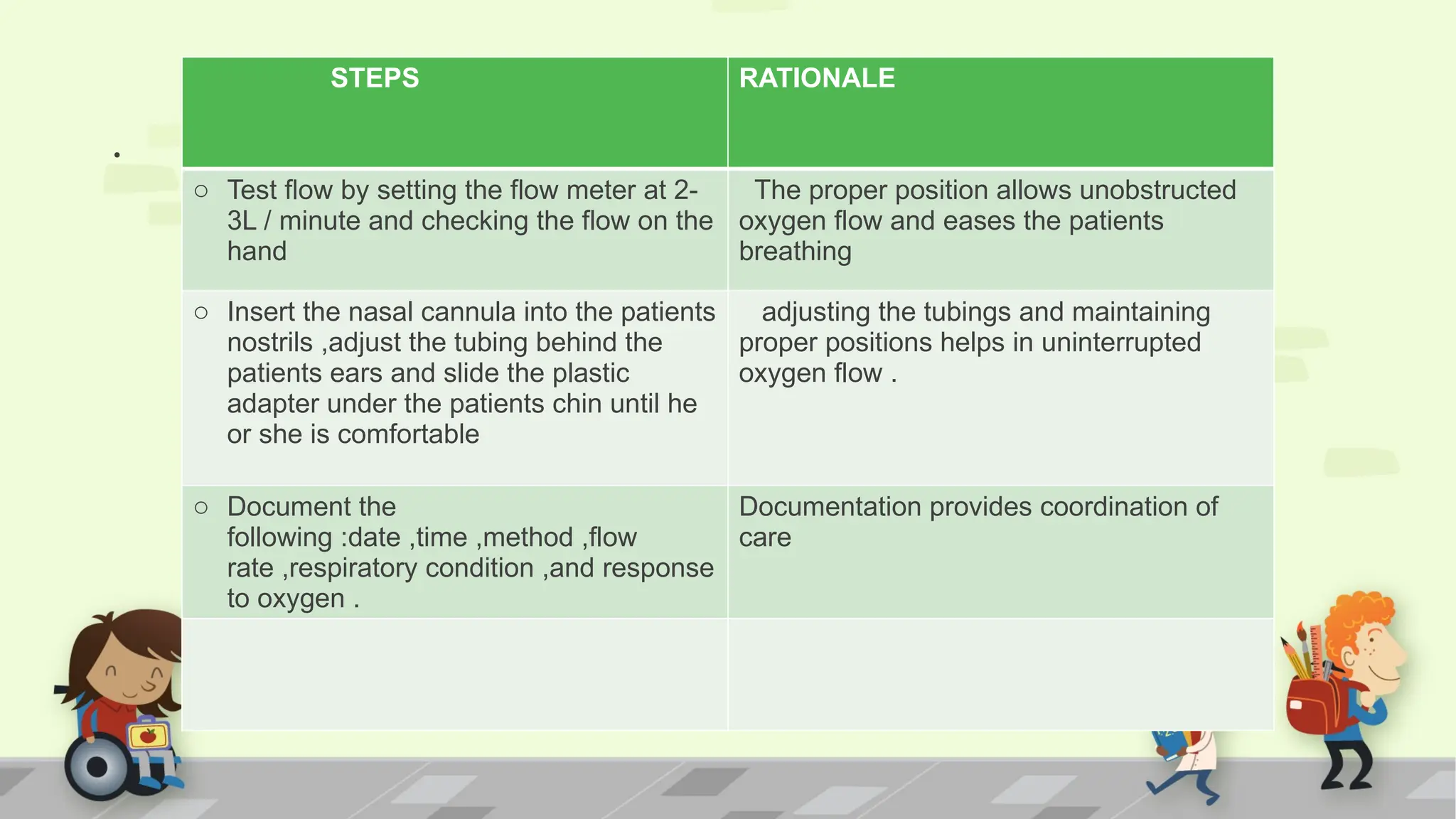
STEPS RATIONALE
o Testflow by setting the flow meter at 2-
3L / minute and checking the flow on the
hand
The proper position allows unobstructed
oxygen flow and eases the patients
breathing
o Insert the nasal cannula into the patients
nostrils ,adjust the tubing behind the
patients ears and slide the plastic
adapter under the patients chin until he
or she is comfortable
adjusting the tubings and maintaining
proper positions helps in uninterrupted
oxygen flow .
o Document the
following :date ,time ,method ,flow
rate ,respiratory condition ,and response
to oxygen .
Documentation provides coordination of
care
54.
HAZARDS OF OXYGENADMINISTRATION THERAPY
INFECTION
COMBUSTION
DRYING OF MUCOUS MEMBRANES
OXYGEN TOXICITY
ATELECTASIS
APNEA
ASPHYXIA
RETROLENTAL FIBROPLASIA
.
• lt isthe procedure where the tracheobronchial
secretions are suctioned out when the coughing reflex
is ineffective or absent.
.Purposes
• To remove secretions that obstruct the airway.
• To facilitate ventilation.
• To obtain secretions for diagnostic purposes.
• To prevent infection that may result from accumulated
secretions.
57.
.
ASESSMENT
Assess for clinicalsigns indicating the need for suctioning. They
are,
• Restlessness, gurgling sounds during respiration.
• Adventitious sounds when the chest is auscultated.
• Change in mental status
• Change in skin color
• Rate and pattern of breathing.
• Decreased oxygen saturation
STEPS OF PROCEDURE
•Explain the procedure to the patient
• Provide privacy
• Collect the articles at the bedside
• Position a conscious person who has a functional gag reflex in a semi-
Fowler's position with the head turned to one side for oral suctioning with the
neck hyperextended for nasal suctioning
• ,Set the pressure on the suction gauge and turn on the suction.
• .Many suction devices are calibrated to three pressure ranges.
• Wall unit:
• .Adult: 80 to 120 mmHg
• Infants and Children: 80 to 100 mmHg
60.
.
• . Newborn:60 to 100 mmHg
ORAL AND OROPHARYNGEAL SUCTION
1. With your sterile gloved hand, pick up the catheter and attach it to the
suction unit
Moisten the tip of the suction catheter with sterile saline water.
Rationale: This reduces friction.
2) Pull the tongue forward, if necessary, using gauze. Do not apply suction
Rationale: Applying suction during insertion causes trauma to the mucous
membranes.
3) Test the pressure of the suction and the patency of the catheter.
Applying your sterile gloved thumb to the port or open branch of the Y-
connector to create suction.
61.
.
4. Advance thecatheter about 10-15 cm (4 to 6 inches)along oneside of the
mouth into the oropharynx
Rationale; Directing the catheter along the side prevents gagging
5. Gentle rotation of the catheter ensures that all surfaces are reached and
prevents trauma
6. Apply suction for 5-10 seconds while slowly withdrawing the catheter
7. Then remove the finger from the control and remove the catheter
8. Rinse the catheter and repeat suctioning
9. Allow sufficient time between each suction
10. Document the procedure
62.
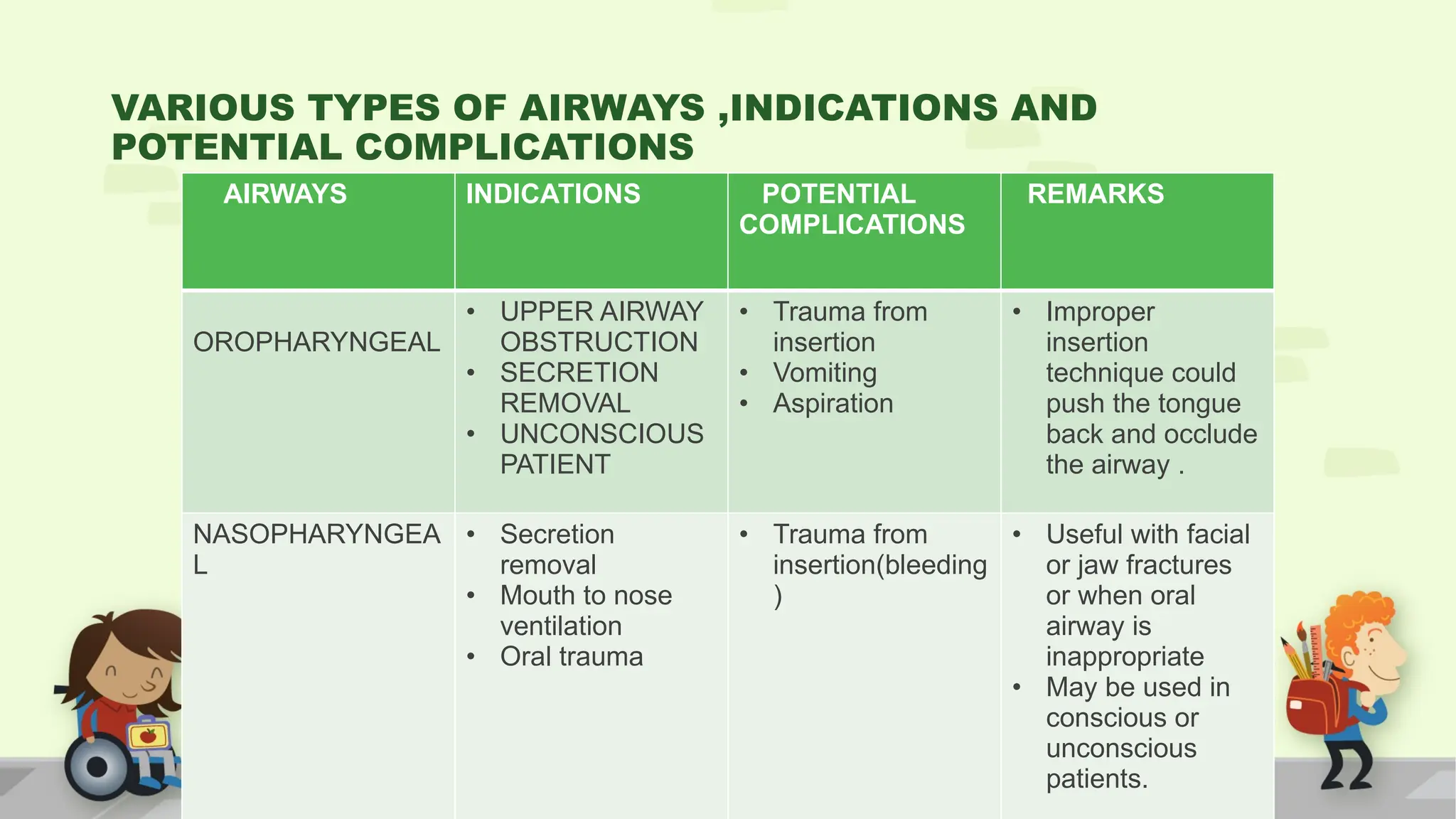
VARIOUS TYPES OFAIRWAYS ,INDICATIONS AND
POTENTIAL COMPLICATIONS
AIRWAYS INDICATIONS POTENTIAL
COMPLICATIONS
REMARKS
OROPHARYNGEAL
• UPPER AIRWAY
OBSTRUCTION
• SECRETION
REMOVAL
• UNCONSCIOUS
PATIENT
• Trauma from
insertion
• Vomiting
• Aspiration
• Improper
insertion
technique could
push the tongue
back and occlude
the airway .
NASOPHARYNGEA
L
• Secretion
removal
• Mouth to nose
ventilation
• Oral trauma
• Trauma from
insertion(bleeding
)
• Useful with facial
or jaw fractures
or when oral
airway is
inappropriate
• May be used in
conscious or
unconscious
patients.
63.
.
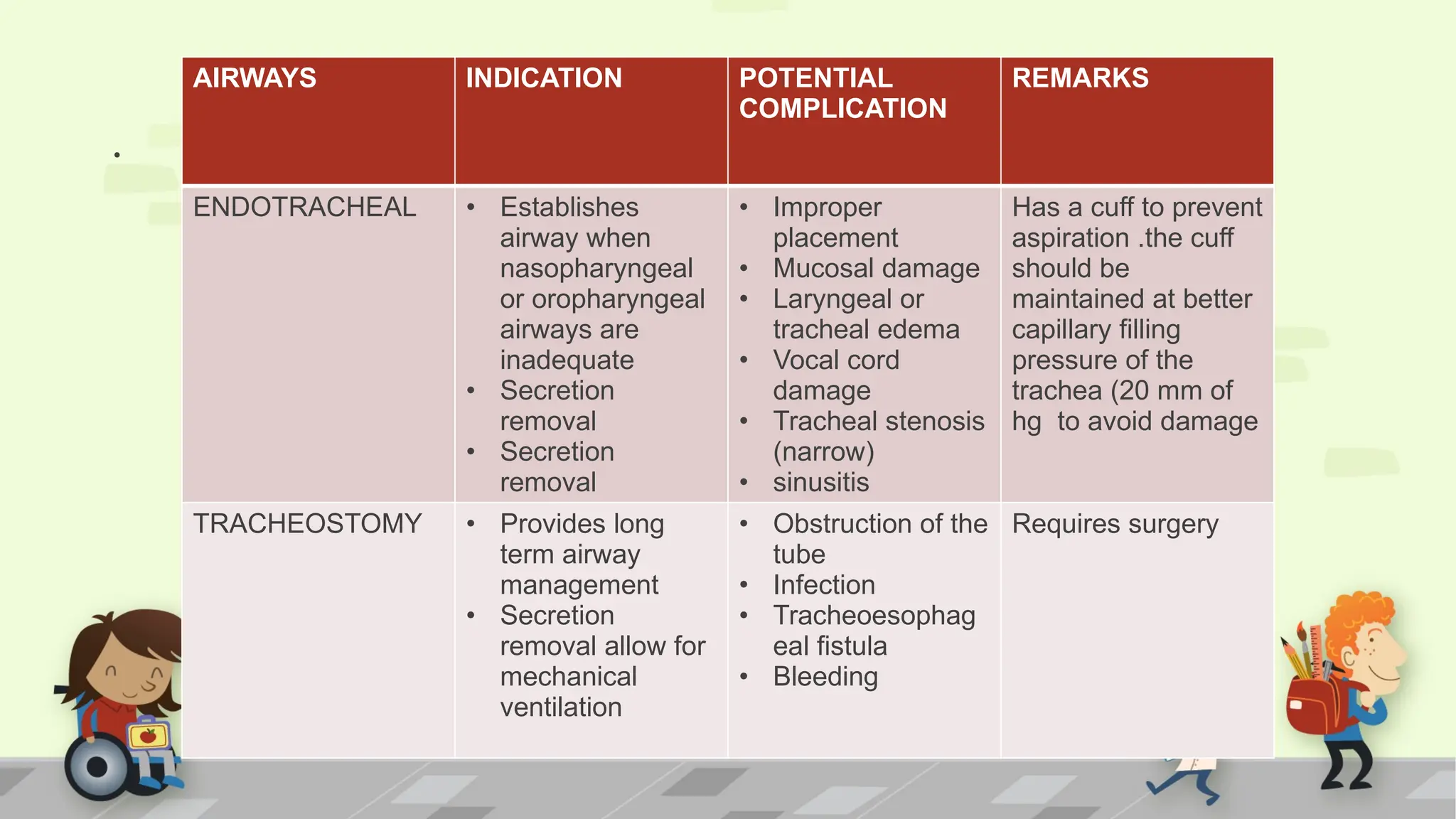
AIRWAYS INDICATION POTENTIAL
COMPLICATION
REMARKS
ENDOTRACHEAL• Establishes
airway when
nasopharyngeal
or oropharyngeal
airways are
inadequate
• Secretion
removal
• Secretion
removal
• Improper
placement
• Mucosal damage
• Laryngeal or
tracheal edema
• Vocal cord
damage
• Tracheal stenosis
(narrow)
• sinusitis
Has a cuff to prevent
aspiration .the cuff
should be
maintained at better
capillary filling
pressure of the
trachea (20 mm of
hg to avoid damage
TRACHEOSTOMY • Provides long
term airway
management
• Secretion
removal allow for
mechanical
ventilation
• Obstruction of the
tube
• Infection
• Tracheoesophag
eal fistula
• Bleeding
Requires surgery































































































![Oxygenation 1st yr corrected 02 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/oxygenation1styrcorrected02autosaved-250107063557-199b5b45-thumbnail.jpg?width=640&height=640&fit=bounds)






































